






VHA Diagnostic Electron Microscopy Program



Examples of Diagnostic Transmission Electron Microscopy (TEM) Cases
Case 1. A 33-year-old man with AIDS presented with fever, nightsweats, generalized lymphadenopathy, and a 30 Ib. weight loss. An inguinal lymph node biopsy was performed. There was no consensus as to the diagnosis among the pathologists who studied H&E sections of the biopsy. An obscure infectious disease, a B-cell lymphoma with amyloid stroma, and possibly Hodgkin's disease were the major considerations. TEM study revealed unexpected clusters of small, pleomorphic, coccobacillary bacteria in vascular walls typical of cat scratch disease. These bacteria were later further identified by polymerase chain reaction as belonging to the genus Rochalimaea (now Bartonella), an important cause of cat scratch disease.
Bacteria are prokaryotes and lack membrane-bound organelles, especially membrane bound nuclei. They have a cell wall of variable thickness. In Figure 1 a cluster of small, pleomorphic bacteria with thin cell walls is present in an area of degeneration with fibrin deposition. In Figure 2 the bacteria have invaded the wall of a capillary.
Reference: Ultrastructural Pathology 20:195-202, 1996.
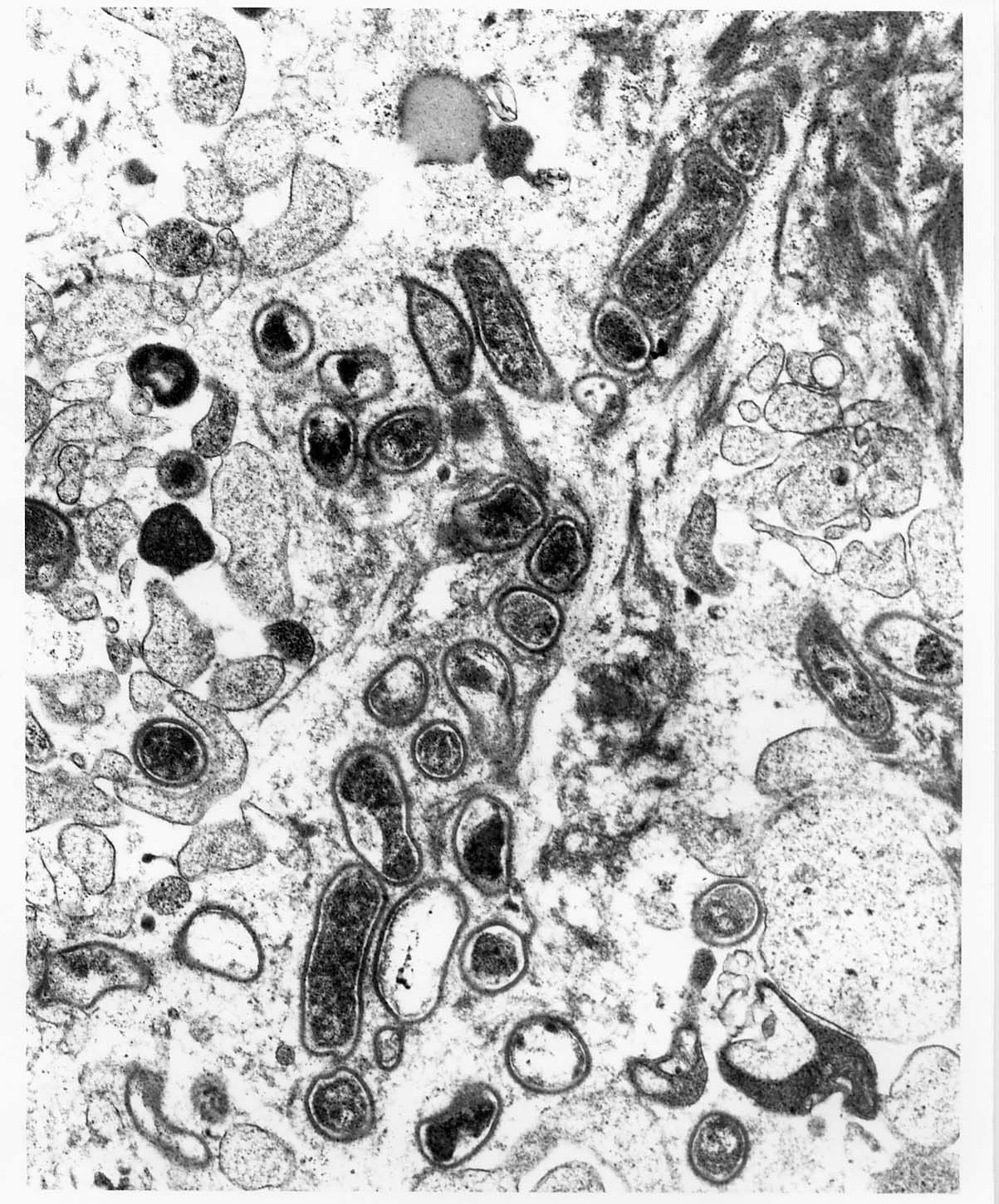
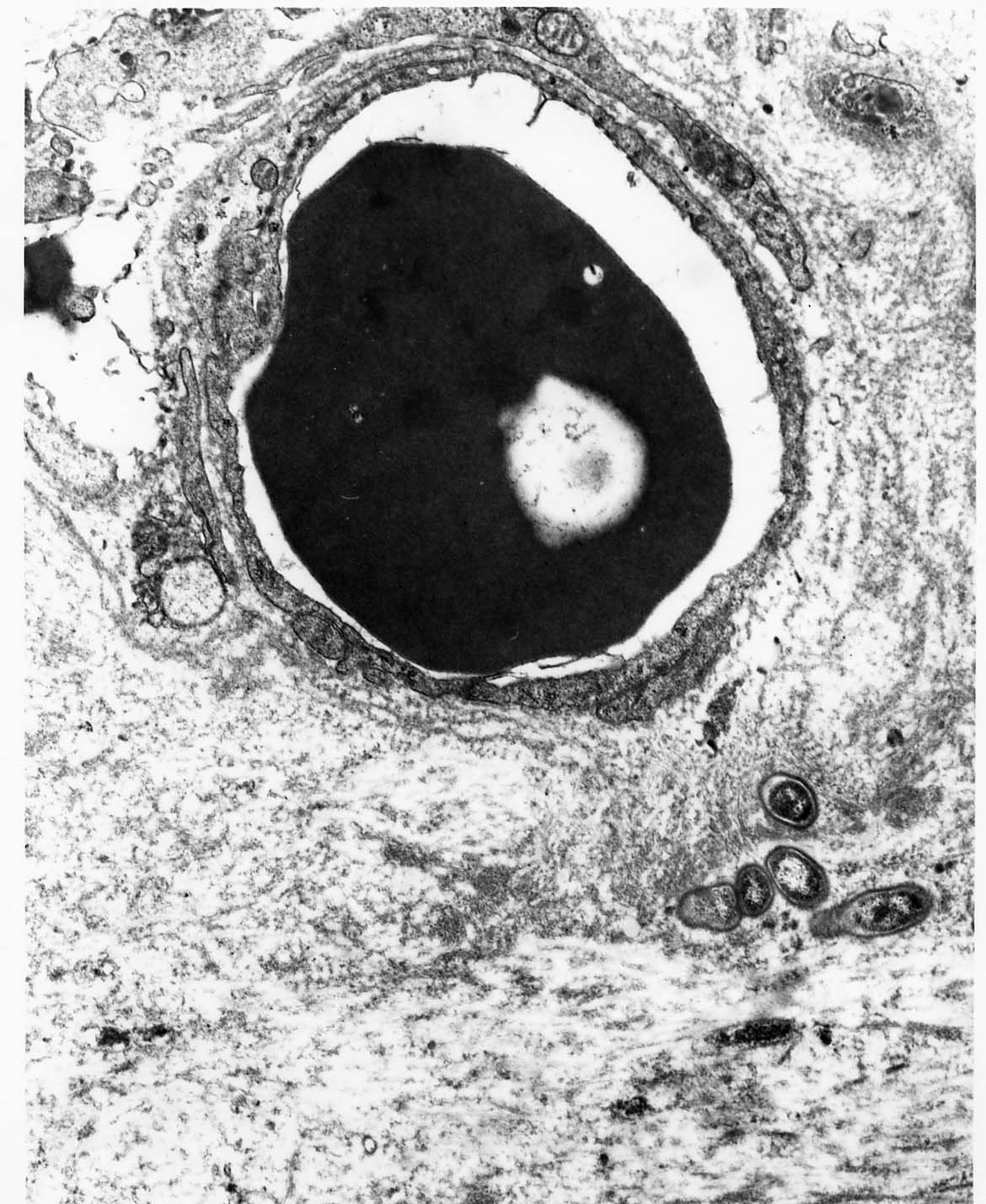
Case1 Fig1 Case1 Fig2
ACUTE DISSEMINATED TOXOPLASMOSIS
Case 2. A 43-year-old man with AIDS developed septic shock and disseminated intravascular coagulation and died five days later. Blood cultures had no growth. The etiology of the patient's sepsis and death was unknown. A bone marrow biopsy performed the day of the patient's demise revealed numerous, very small, bluish bodies in hematopoietic cells. The differential diagnosis for intracytoplasmic bluish bodies included Histoplasma capsulatum, Toxoplasma gondii, Leishmania donovanii, microsporidia, and Ehrlichia chaffeensis. Pathologists and microbiologists differed in their opinions as to the exact nature of the infectious agent and it became apparent that acccurate identification of the organism could not
be accomplished by LM alone. TEM study of the bone marrow revealed the longitudinally sectioned organisms to have a conoid and rhoptries characteristic of tachyzoites of Toxoplasma gondii . Thus this AIDS patient had acute disseminated toxoplasmosis.
Protozoa, including Toxoplasma gondii are eukaryotes and have membrane-bound organelles, especially membrane-bound nuclei. Protozoa do not have double layered cell walls, whereas fungi do. In Figure 1 several haphazardly sectioned tachyzoites have invaded a hematopoietic cell, probably a plasma cell. In Figure 2 a conoid (arrowheads) is present at the anterior end of the longitudinally sectioned tachyzoite. In Figure 3 several rhoptries (R) or glands are present in a tangentially sectioned tachyzoite.
Reference: Ultrastructural Pathology 19:95-99,1995.

 is present at the anterior end of the longitudinally sectioned")
 or glands are present in a tangentially sectioned tachyzoite.")
Case2 Fig1 Case2 Fig2 Case2 Fig3
Case 3. A 40-year-old, male, AIDS patient presented with an extensive facial ulcer. A biopsy of the ulcer suspected of being herpetic in nature did not reveal typical herpetic changes by LM and immunohistochemical studies had equivocal results. TEM study of the skin biopsy revealed numerous herpesvirus nucleocapsids in the nuclei of necrotic keratinocytes (Figure 1). A viral culture of the facial ulcer subsequently confirmed the diagnosis of herpetic cutaneous infection.
In Figure 2 the nucleocapsids of the herpesvirus present in the nucleus of a necrotic keratinocyte typically have electron dense, homogeneous cores surrounded by membrane-like capsids. In Figure 3 several enveloped nucleocapsids are present in the degenerated keratinocyte cytoplasm.
. A viral culture of the facial ulcer subsequently confirmed the diagnosis of herpetic cutaneous infection.")


Case3 Fig1 Case3 Fig2 Case3 Fig3
Case 4. A 55-year-old, HIV+ man presented with an erythematous papular rash on his chest and back of four years duration. Pityriasis rosea was favored by the dermatologist and a skin biopsy was considered compatible with that diagnosis. A dermatopathologist noted conspiciuous plasma cells in dermal, perivascular cellular infiltrates and suggested the possibility of syphilis. The dermatologist considered this diagnosis unlikely, since the rash had been apparently present for four years and
a serologic test for syphilis (Rapid Plasma Reagin) performed three months before the skin biopsy was negative. TEM study of the skin biopsy (performed initially to rule out vascular injury as part of a possible drug eruption) unexpectedly showed spirochetes in the walls of dermal blood vessels. This finding together with the conspicuous plasma cells in the dermal infiltrates was highly suggestive of syphilis and a repeat serologic test for syphilis was strongly recommended. The repeat Rapid Plasma Reagin test was positive to a dilution of 1:64. Infectious disease specialists subsequently examined the patient and found that the rash had been present for four weeks (not four years) and it also involved the patient's palms and soles. These findings were considered typical of secondary syphilis and the patient was treated with long acting bicillin.
Spirochetes are helical bacteria (prokaryotes) and lack membrane-bound organelles. They have distinctive, linear, electron dense, axial fibrils which are located between their protoplasmic cylinders and plasma membranes and aid in electron microscopic recognition of spirochetes in ultrathin tissue sections. In Figure 1 two spirochetes (arrowhead) are present in the wall of a dermal blood vessel. In Figure 2 their resemblance (arrowhead) to cytoplasmic processes of host cells is apparent. In Figure 3 clusters of tangentially sectioned axial fibrils (arrowhead) are present in the spirochetes and aid in their identification.
 are present in the wall of a dermal blood vessel.")
 to cytoplasmic processes of host cells is apparent.")
 are present in the spirochetes and aid in their identification.")
Case4 Fig1 Case4 Fig2 Case4 Fig3
ACUTE DISSEMINATED HISTOPLASMOSIS
Case 5. A 53 year old, black man with a history of AIDS and a CD4 lymphocyte count of 4 presented with hypotension, acute renal failure, a LDH of 10, 050, a SGOT of 1940, and a CPK of 2,014. Microorganisms suggestive of Histoplasma capsulatum were observed in peripheral blood smears.Ultrastructural study of the buffy coat of peripheral blood revealed small yeasts consistent with Histoplasma capsulatum both extracellularly and within neutrophils and macrophages. A urine test for Histoplasma capsulatum antigen was positive. The patient died on the second day of his illness.
This patient's clinical picture of acute disseminated histoplasmosis was quite similar to the clinical picture of acute disseminated toxoplasmosis in Case 1. In Figure 1 a yeast is present in the extracellular space and has a typical, multilayered (alternating light and dark layered) cell wall and membrane-bound organelles including a membrane-bound nucleus and mitochondria. In Figure 2 a yeast with a single bud is present in a neutrophil.
 cell wall and membrane-bound organelles including a membrane-bound nucleus and mitochondria.")

Case5 Fig1 Case5 Fig2
BACTERIAL ENTERITIS IN AN AIDS PATIENT WITH INTESTINAL CYTOMEGALIC INCLUSION DISEASE AND INTESTINAL MICROSPORIDOSIS
Case 6. A 45 year old, HIV+ man presented with chronic diarrhea. Terminal ileal and colonic biopsies were obtained and light microscopy showed only mild chronic inflammation and no microorganisms. Electron microscopic study of the ileal and colonic biopsies revealed three infectious agents and diseases not seen light microscopically: bacterial enteritis, cytomegalic inclusion disease, and microsporidiosis.
In Figure 1 the adherence and effacement lesion (A&E lesion) caused by enteropathogenic Escherichia coli (grown on stool culture) is shown. Several rod shaped bacteria are adherent to the plasma membranes of colonic enterocytes which also have effacement or loss of their microvilli. In Figures 2 and 3 a cytomegalic endothelial cell of a blood vessel in the colonic lamina propria has a small intranuclear inclusion body containing nucleocapsids typical of a herpesvirus. In Figure 4 a degenerated enterocyte at the tip of an ileal mucosal villus contains a late sporont of a microsporidium. A higher magnification of a late sporont is present in Figure 5. It is dark staining and contains multiple nuclei and several developing polar tubes. In contrast, early sporonts are light staining and contain multiple nuclei and scattered, lucent slits, but no developing polar tubes.
 caused by enteropathogenic Escherichia coli (grown on stool culture) is shown. Several rod shaped bacteria are adherent to the plasma membranes of colonic enterocytes which also have effacement")



Case6 Fig1 Case6 Fig2 Case6 Fig3 Case6 Fig4
 Case6 Fig5
Case6 Fig5
TRICHOMONIASIS COMPLICATING ESOPHAGEAL INTRAMURAL PSEUDODIVERTICULITIS
Case 7. A 58-year-old African-American man presented with a progressive esophageal stricture of unknown etiology complicated by esophageal candidiasis, broncho-esophageal fistula, four episodes of aspiration pneumonia, and a 40 Ib weight loss. He ultimately required an esophagectomy. Pathologic examination showed marked thickening of the esophageal wall by submucosal pseudodiverticula typical of esophageal intramural pseudodiverticulosis (EIPD) and extensive mucosal and submucosal chronic inflammation and fibrosis. Small, oval cells with ill-defined nuclei were present in lumens of some pseudodiverticula, light microscopically. Their exact nature was not known by light microscopy. The diagnosis of trichomoniasis became apparent only after transmission electron microscopic study of these cells demonstrated characteristic features of trichomonad protozoa. These included four anteriorly-placed flagella with kinetosomes, a recurrent flagellum associated with an undulating membrane, a costa, a peltar-axostylar complex, and a small Golgi body with parabasal filaments.
Figure 1 shows two trichomonads, one being to the right of center and the other on the left side. A squamous epithelial cell (S) is above them.
Axostyles (arrows), nucleus (N), four anteriorly placed flagella in cross section (larger arrowhead), and hydrogenosomes (smaller arrowheads) are present in the trichomonads. Figure 2 shows a trichomonad (center) partially surrounded by squamous epithelial cells (S). An axostyle (arrow), nucleus (N), two anteriorly placed flagella (larger arrowhead), costa (smaller arrowhead), and hydrogenosomes (H) are present in the trichomonad.
Reference:Ultrastructural Pathology 1996;20:101-107.

 partially surrounded by squamous epithelial cells (S).")
Case7 Fig1 Case7 Fig2
Case 8. A 48-year-old, African-American man with AIDS presented with alternating watery diarrhea and constipation of one month duration. The purpose of the EM study of the biopsied colonic hyperplastic polyp was to help determine the cause of the patient's alternating diarrhea and constipation. Ultrastructurally, a dense growth of spirochetes covered the mucosal epithelial surface of the biopsied colonic hyperplastic polyp (Figures 1 and 2). The basophilic fringe typical of intestinal Ispirochetosis was present light microscopically in this case, but was not initially appreciated by both the surgical pathologist and the electron microscopist. The patient's alternating watery diarrhea and constipation ceased after removal of two colonic hyperplastic polyps and were probably functional in nature. The intestinal spirochetosis diagnosed by EM in this case was probably an incidental finding and probably did not cause the patient's symptoms. In Figure 3, high magnification (X46/000) of cross-sectioned spirochetes reveals groups of four and eight axial fibrils (arrowheads) in the periplasmic space between the protoplasmic cylinder and the plasma membrane of the spirochetes. In a longitudinally sectioned spirochete, the axial fibril (arrow) appears as a linear density in the periplasmic space. Recognition of the axial fibrils aids in ultrastructural identification of spirochetes in tissue. The spirochetes present in this case were subsequently identified as Brachyspira aalborgii (2).
References: 1. Ultrastructural Pathology, 1995;19:15-22.
2. Journal of Clinical Microbiology, 1999:37:2093-2098.
.")
.")
 of cross-sectioned spirochetes reveals groups of four and eight axial fibrils (arrowheads)")
Case8 Fig1 Case8 Fig2 Case8 Fig3
PULMONARY BLASTOMYCOSIS IN AN AIDS PATIENT
Case 9. A 42-year-old, African-American man presented with a two month history of weight loss and fever for two weeks. Presumptive diagnoses of human immunodeficiency virus infection (HIV) and acquired immunodeficiency syndrome were made on the basis of a CD4 lymphocyte count of 23 lymphocytes/ml. Chest X-ray revealed right paratracheal adenopathy and a miliary pattern. The etiology of the patient's pulmonary infection was not known, but tuberculosis was an important consideration. Over five days, the pulmonary infection progressed and was complicated by acute respiratory distress syndrome (ARDS), septic shock, and death despite vigorous antibiotic and supportive therapy. Serologic tests for HIV infection were reported as positive after the patient's demise. The etiology of the patient's pulmonary infection, ARDS, and sepsis was not known until autopsy study revealed enumerable yeast-like cells of Blastomyces dermatitidis in the extensively consolidated lungs and in disseminated foci of infection in most other major organs. Diffuse alveolar damage was closely associated with the pulmonary blastomycosis. Electron microscopic study of the yeast-like cells (Figures 1 & 2) of B. dermatitidis in the autopsy lung obtained and fixed five days after the patient's death revealed excellent preservation of viable organisms. The yeast-like cells of Blastomyces dermatitidis typically have multiple (3-5) nuclei (Figure 1) and a cell wall with alternating light and dark layers (Figure 2).
Reference: Ultrastructural Pathology 1996;20:429-435.
 nuclei (Figure 1)")
.")
Case9 Fig1 Case9 Fig2
Case 10. A 39-year-old, homosexual, Caucasian man with a nine month history of acquired immunodeficiency syndrome by reduced CD4 lymphocyte count alone was found to have extensive, asymptomatic, nonremovable, corrugated, white patches on the lateral borders and ventral aspects of the tongue typical of oral hairy leukoplakia (OHL). Histologically, irregular hyperparakeratosis, acanthosis, and clusters of ballooned kertinocytes in the stratum spinosum were present in the biopsied lateral tongue. Some of the superficial ballooned keratinocytes had peripherally beaded nuclei, whereas others had ground glass intranuclear inclusions. Ultrastructurally, the ballooned keratinocytes had three important findings of diagnostic significance. First, frequent herpesvirus nucleocapsids were largely confined to superficial ballooned keratinocytes having marginated and condensed chromatin (Figure 1). In searching for herpesvirus nucleocapsids, the marginated and condensed chromatin was an invaluable marker for cells harboring the virions. Second, the marginated and condensed chromatin frequently had a distinctive punched-out (Figure 1) or cribriform appearance (Figure 2). Third, the ground glass intranuclear inclusion bodies consisted of central, medium electron dense, finely granular material containing frequent herpesvirus nucleocapsids and partially surrounded or capped by prominent, clumped chromatin (Figure 3). The patient died with progressive multifocal leukoencephalopathy 24 months after OHL was diagnosed.
Reference: Ultrastructural Pathology 1999;23:181-187.
.")
 or cribriform appearance (Figures 2).")
.")
Case10 Fig1 Case10 Fig2 Case10 Fig3
PULMONARY CRYPTOCOCCOMA
Case 11. A 63 year old, black man with a history of head and neck cancer was found to have a nodule in his lower lobe, right lung (RLL). H&E sections of a CT-guided, needle biopsy of the RLL nodule initially revealed only fibrosis and not the suspected carcinoma. Semithin sections of minute bits of the biopsy revealed several, obvious, round yeast-like structures in minute, non-caseous granulomas and several multinucleated giant cells. These microorganisms were virtually invisible and missed in the H&E sections, but were readily apparent in subsequently prepared GMS sections (indicated by the initial EM study). Ultrastructurally, several yeasts had prominent capsules with radiating, corona-like fibrillar material typical of Cryptococcus (Figures 1, 2, & 3). A positive mucicarmine stain subsequently confirmed the diagnosis of cryptococcosis. The patient is being followed for his cryptococcoma. This diagnosis would have been missed if it were not for the EM study and the patient was spared a thoracotomy and surgical resection of the RLL nodule because of the EM study.
.")
.")
.")
Case11 Fig1 Case11 Fig2 Case11 Fig3
DISAPPEARING INTESTINAL SPIROCHETOSIS
Case 12. A 32-year-old man presented with a six-year history of chronic bloating, crampy lower abdominal pain, and watery diarrhea with up to 10 bowel movements per day. All laboratory studies were negative. Physical examination was unremarkable, as were esophagogastroduodenoscopy and two colonoscopies. However, biopsies of the colonic muocsa obtained during the first colonoscopy revealed intestinal spirochetosis. Light micrscopy showed the typical basophic band covering the colonic epithelial surface with a mild chronic inflammatory reaction in the lamina propria. Electron microscopy revealed the basophilic band to consist of a dense growth of spirochetes adjacent to and oriented perpendicular to the surface of the colonic muocsal epithelium. The spirochetes measured 4-5 micra long and contained four to eight periplasmic fibrils. With persistence of the diarrhea for six weeks without antibiotic therapy, a second colonoscopy was performed and biopsies at this time showed disappearance of the basophilic band by light microscopy and with it the corresponding dense growth of spirochetes by electron microscopy, but electron microscopy also showed sparse spirochetes had invaded the mucosal epithelium and were present in goblet cells (Figures 1 & 2) and enterocytes. Subsequent treatment with metronidazole 500 mg four times a day for 10 days resulted in marked clinical improvement within a week. This improvement persisted for four months after which time the patient was lost fo follow-up.
Reference: Digestive Diseases and Sciences. 2000;45:1006-1010.
 and enterocytes.")
 and enterocytes.")
Case12 Fig1 Case12 Fig2






