









Building Trust to Advance Veteran Health Equity
Building Trust to Advance Veteran Health EquityJessica Marshall, MPH(c), Office of Health Equity, Lauren Korshak, DHealth(c), MS, RCEP, Office of Health Equity, Juliette McClendon, PhD, National Center for PTSD and VA Boston Health Care System, Shannon Jordan, MPH, Office of Health Equity |
 |
Download PDF
INTRODUCTION
Equitable access to high-quality care for all Veterans is a major tenet of the VA health care mission, and the Office of Health Equity (OHE) champions the elimination of health disparities to achieve health equity for all Veterans.
VA health care providers support the Veterans Health Administration’s (VHA) mission, and believe it is both their own and VHA’s responsibility to eliminate health disparities among Veterans. An essential aspect of advancing health equity is actively working to gain greater trust from Veterans, especially individuals from marginalized groups (e.g., racial, ethnic and sexual minorities).
CHALLENGES TO TRUSTING HEALTH CARE PROVIDERS
People who have reported that they’ve experienced discrimination also have lower trust in medical providers and may be less likely to trust their health care system. This can lead to poor health care outcomes and health disparities.
Work by researchers at the Boston VA and Washington University in St. Louis suggests that trust is eroded among Black Americans in part in reaction to experiences of discrimination, such as being denied a loan or housing because of one’s race, gender, or other marginalized identity.
Additional VA research has found that a significant portion of Veterans of Color have experienced discrimination in health care, which is linked to lower satisfaction with and perceived quality of care as well as worse health outcomes.
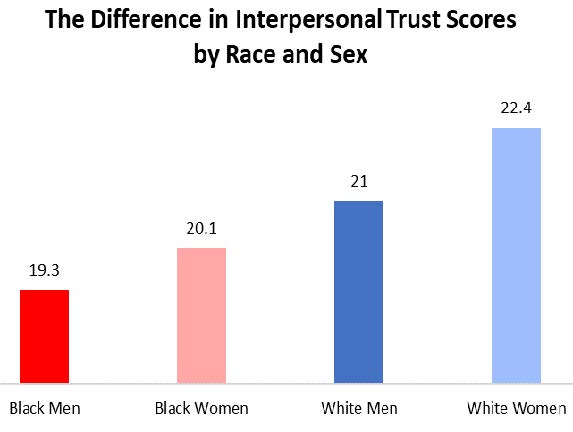
*Trust scores are from the NEO Personality Inventory
From: McClendon, J., et al. (2019). Mechanisms of Black-White disparities in health among older adults: Examining discrimination and personality. Journal of Health Psychology.
ADDRESSING DISCRIMINATION AND BUILDING TRUST
VA is working hard to ensure that VA health care providers can recognize and address any unconscious biases that may influence their interactions with patients and staff. The Office of Health Equity (OHE) provides several online trainings on unconscious bias, as well as other topics centered on cultural competence.
In the trainings on unconscious bias, VHA providers share their stories of creating awareness of unconscious bias within their clinical practice and how bias impacts us all. A bias is a tendency. Most biases are natural. However, biases can cause problems when we are not aware of them and we apply them inappropriately to our everyday choices, which can lead to discriminatory practices and result in poorer health outcomes and experiences for patients.
The ACORN (Assessing Circumstances and Offering Resources for Needs) Implicit Bias Training Guide is also available through OHE’s website. It was developed by VA Boston Healthcare System in Massachusetts and serves as a review on implicit bias and how it can indirectly affect VA providers’ care, as well as provides tools and strategies for how providers and clinicians can reduce their own biases. Continued acknowledgement and active practice to reduce implicit bias is an essential role in advancing health equity.
In addition to resources available through OHE, the Office of Resolution Management, Diversity & Inclusion compiled a set of diversity trainings on implicit bias, inclusion, cultural competence, micro-behaviors, and other topics that help eliminate discrimination and foster a welcoming environment which builds trust. Available to VA employees, these trainings include mandatory trainings, The Prevention of Workplace Harassment and No FEAR Act and EEO, Diversity, Conflict Management Training for Managers and Supervisors, as well as access to additional on demand and instructor led trainings.
The Office of Health Equity's online trainings and unconscious bias and cultural competence trainings can be found here.
The Office of Resolution Management, Diversity & Inclusion online trainings can be found here (VA network TMS 2.0 only).
For more information about the Office of Health Equity visit: https://www.va.gov/healthequity.
REFERENCES:
Brondolo E, Hausmann LRM, Jhalani J, et al. (2011). Dimensions of perceived racism and selfreported health: Examination of racial/ethnic differences and potential mediators. Annals of Behavioral Medicine 42(1): 14–28.
Hausmann LR, Kressin NR, Hanusa BH, Ibrahim SA. Perceived racial discrimination in health care and its association with patients' healthcare experiences: does the measure matter?. Ethn Dis. 2010 Winter;20(1):40-7.
Hausmann LR, Gao S, Mor MK, Schaefer JH Jr, Fine MJ. Understanding racial and ethnic differences in patient experiences with outpatient health care in Veterans Affairs Medical Centers. Med Care. 2013 Jun;51(6):532-9.
McClendon, J., Perkins, D., Copeland, L., Finley, E. and Vogt, D. (2019). Patterns and correlates of racial/ethnic differences in posttraumatic stress disorder screening among recently separated Veterans. Journal of Anxiety Disorders, 68, 102-145.
McClendon, J., Bogdan, R., Jackson, J.J., and Oltmanns, T.F. (2019). Mechanisms of Black-White disparities in health among older adults: Examining discrimination and personality. Journal of Health Psychology.
Rickles, N., et al. (2010). Perceptions of Healthcare, Health Status, and Discrimination Among African-American Veterans. Journal of Health Disparities Research and Practice, 4 (2)






