Attention A T users. To access the menus on this page please perform the following steps.
1. Please switch auto forms mode to off.
2. Hit enter to expand a main menu option (Health, Benefits, etc).
3. To enter and activate the submenu links, hit the down arrow.
You will now be able to tab or arrow up or down through the submenu options to access/activate the submenu links.
Whole Health emphasizes mindful awareness and Veteran self-care, in addition to excellent professional care. The Circle of Health highlights Food and Drink and its relationship to the other areas of self-care: Surroundings; Personal Development; Recharge; Family Friends, and Co-workers; Spirit and Soul; Power of the Mind; and Moving the Body.
A Whole Health approach to nutrition also incorporates complementary and integrative practices to prevent or improve acute and chronic symptoms related to cardiovascular disease, diabetes, gastrointestinal diseases, mental health, and chronic pain. Nutrition is a vast area, and while this overview cannot cover every option a Veteran can consider, it provides a starting place, building on the material provided in Chapter 8 of the Passport to Whole Health. Whether someone chooses to add in a food or food group, remove something from their diet, or change a behavior, focusing on nutrition can have a profound impact on health. The narrative below shows what a Whole Health clinical visit could look like and how to apply the latest research on complementary and integrative health (CIH) to dietary recommendations.
Key Points
The Standard American Diet (SAD) does not provide us with optimal nutrients. Poor eating habits associated with this diet have a profound impact on our health.
Clinicians should individualize care to meet Veterans where they are at; even small changes can lead to good results.
People often are put off by the word “diet.” This overview focuses on a number of “eating plans” that are popularly followed, noting some of the pros and cons of several of them. Remember, a plan’s success is much more likely if the person persists; tying in the benefits of healthy eating to what really matters to a person can be extremely helpful. Be cautious when it comes to fad diets.
Enlist the assistance of dietitians as part of the Whole Health care team. They can be an incredible resource.
When it comes to food safety, pay attention to the Dirty Dozen™ and Clean 15™ guidelines on the Environmental Working Group website.
Meet the Veteran: Erin
“The food you eat can be the safest and most powerful form of medicine or the slowest form of poison.” –Ann Wigmore
Erin is a 35-year-old Navy Veteran and mother of two. Currently, she is overweight, with a body mass index (BMI) of 29. She often feels tired, struggles with constipation, and has some symptoms of gastritis. She also notes frequent migraines and chronic sinus infections. Erin does not have diabetes, but her doctor is concerned because her fasting glucose is elevated, and she has a strong family history of type 2 diabetes.
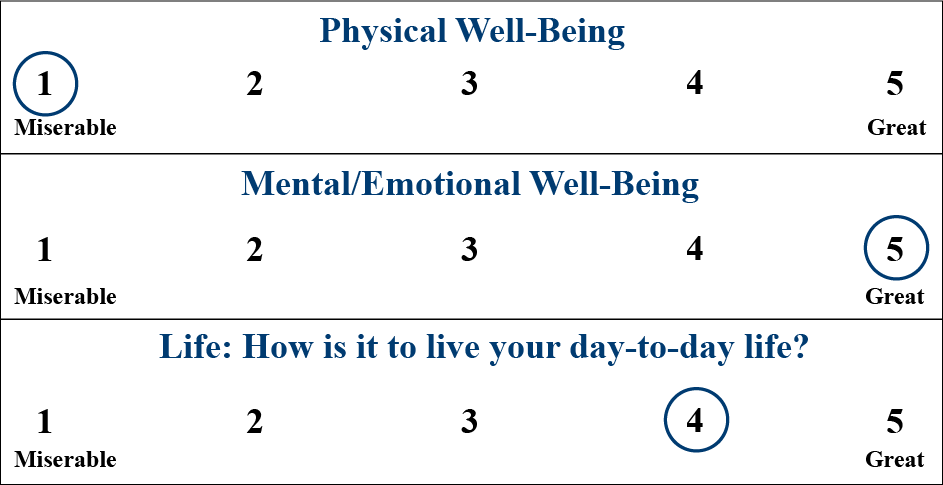
During a recent visit, Erin completed a Brief Personal Health Inventory (PHI). Her care team members reviewed it and noted several areas of concern, positivity, and interest.
Her PHI vitality signs survey indicated a big difference between how she rates her emotional versus physical well-being:
Rate where you feel you are on the scales below from 1-5, with 1 being miserable and 5 being great.
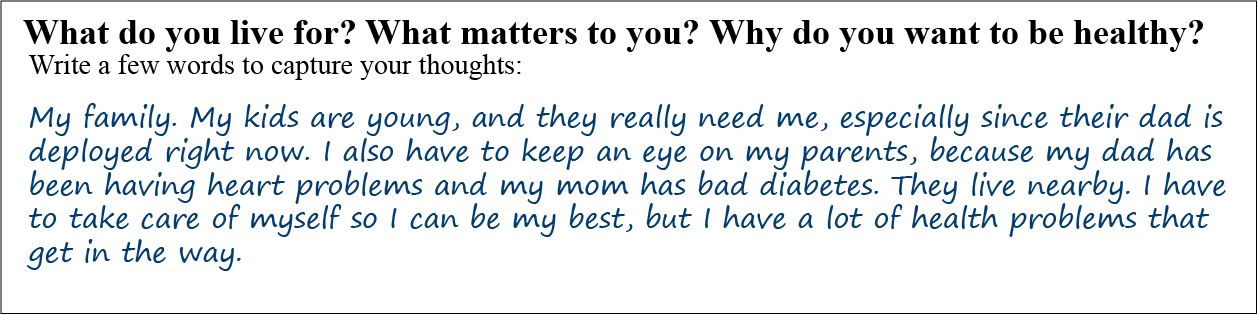
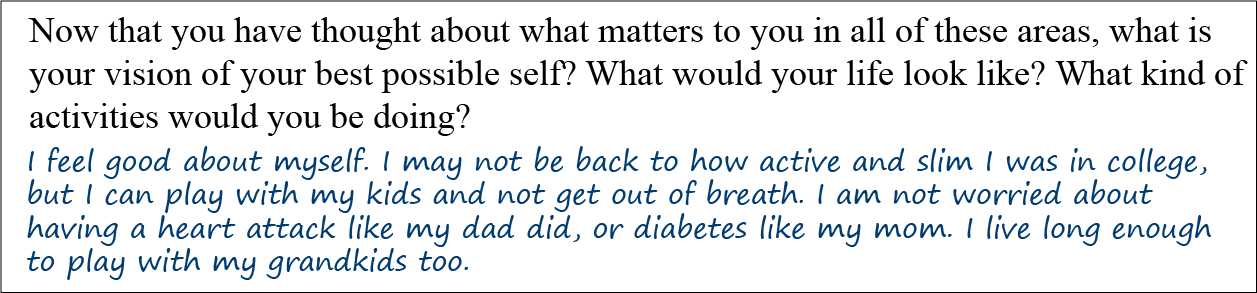
Erin’s Mission/Aspiration/Purpose was centered around her family and her ability to do what she enjoys.
On page 2 of her PHI, Erin reports being where she wants to be in terms of Spirit and Soul, Surroundings, Personal Development, and Family, Friends and Co-workers. Healthy lifestyle and stress reduction are where she seems to have challenges:
Area of Whole Health
Where I Am Now (1-5)
Where I Want to Be (1-5)
Moving the Body
1
5
Recharg
2
5
Food and Drink
0
5
Personal Development
4
4
Family, Friends, and Co-Workers
4
5
Spirit and Soul
5
5
Surroundings
5
5
Power of the Mind
4
5
Professional Care
5
5
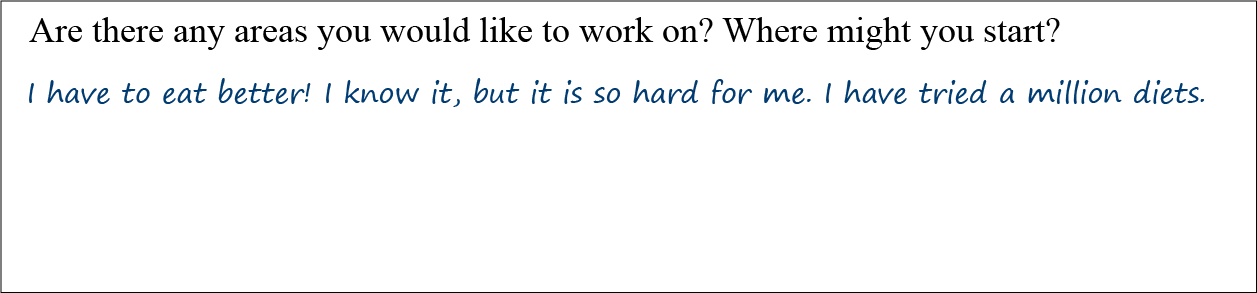
Her “0” out of 5 for Food and Drink was particularly striking, and when asked, Erin agreed that was the area she wanted to work on. She has some initial ideas, but clearly wants some guidance.
During a subsequent visit, Erin provided some information about her diet. Most mornings, she has a bagel or granola bar for breakfast. For lunch, she has leftovers from dinner the night before. Her afternoon snack is usually chips or popcorn. She eats out with her family 3-4 times each week, and she usually chooses a fast food option. She and her children enjoy vegetables, but they only eat a few servings per week. When her family eats at home, they usually eat while watching television. Erin tries to drink mainly water and now avoids beer to cut down on calories. Her teenage son enjoys fruit drinks, so she always stocks the refrigerator with them.
Erin knows she needs to make healthier dietary choices, but she does not know how to go about it. She has the following questions and concerns:
What is the best diet for me to follow? Should I follow a low-fat diet?
What is fiber, and why is it good for me?
What are some good options for protein?
Eating healthy costs too much, and I am not sure I can afford it. Any suggestions?
Juice is high in calories, but it is healthy, right, since it comes from fruit?
Water is boring; are there other things to drink that are good for me?
Sometimes I eat when I am bored or sad, and I know it is not a good way to deal with my feelings, but it makes me feel better. Any ideas?
How do I eat well but still feel satisfied? I hate dieting because I always feel like I am starving.
Should I take a multivitamin?
What minerals do I really need?
Nutrition: An Unpalatable State of Affairs
The prevalence of obesity and overweight in Veterans matches that of the general U.S. population. Eighty-one percent of male Veterans and 54% of female Veterans are overweight or obese (BMI>25). Twenty-five percent of male Veterans and 17% of female Veterans are obese (BMI>30).[1] A 2017 Journal of the American Medical Association study concluded that, in 2012, at least 45.4% of all deaths from heart disease, stroke, and diabetes were ultimately caused by poor diet.[2] The prevalence of overweight and obesity increases every year,[3] and the number of people dying due to poor dietary choices is climbing.[4]
What can be done about the epidemic of unhealthy eating? Many people look to their physicians or other clinicians for nutritional guidance. Little do they know, most clinicians receive limited—even negligible—nutrition training. According to a 2015 survey of 121 medical schools, 71% of schools fail to provide the required 25 hours of nutrition education over 4 years, and 36% of these schools did not provide half that amount.[4] Even more disappointing, courses often lack clinically relevant information that can be applied to patient care. Rather than reviewing research on how to eat well, much of the nutrition curriculum for health professions focuses on biochemistry.
Many patients feel that Food and Drink is an important area of focus for a Personal Health Plan. In fact, many of us tend to fixate on it, even while struggling unsuccessfully with making good dietary choices. Most people know what they should or should not eat. However, they also have a difficult time changing their behaviors in accordance with that knowledge.
As clinicians, the so-called Standard American Diet (SAD) is our nemesis. Erin’s family’s diet is an example of a SAD; it is not a healthy way to eat. The SAD is characterized by the following:[5]
Excessive calorie intake
Too many refined carbohydrates
High consumption of fatty meats
Unhealthy levels of added fats
Limited intake of nutrient-dense foods such as whole grains, fruits, and vegetables
What To Do?
The purpose of this overview and its related Whole Health tools is to provide practical information about nutrition to guide both your own food choices and the nutrition suggestions you offer to your patients. Even if you are pressed for time, it can be beneficial to suggest at least one or two of the nutrition tips offered in this overview during a Whole Health visit. It only takes a few moments, and you can always provide patients with written information that they can review in more detail after their visit. Additionally, you can refer patients to a registered dietitian who can provide in-depth recommendations.
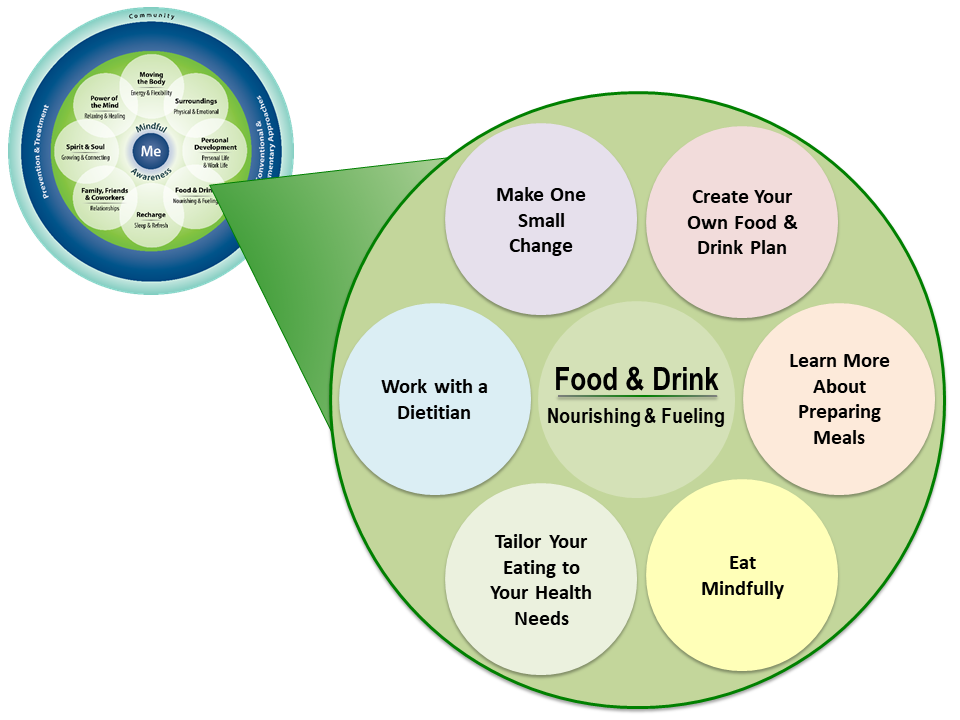
In 2018, VA Office of Patient Centered Care and Cultural Transformation created skills building courses for each of the eight Whole Health self-care topics. Figure 1 illustrates the graphic used for Food & Drink. It offers a series of subtopics that can allow the conversation to go deeper. Note the “Make One Small Change” circle, which leaves room for creativity in any area the Veteran and clinician prefer. Also note the circle that emphasizes “Work with a Dietitian,” acknowledging that they can be an important resource as patients create Personal Health Plans.
Figure 1. Subtopics within the Food & Drink Circle of Self-Care
Patients are more likely to follow nutrition recommendations if they hear them directly form a clinician, and if clinicians can speak to following those recommendations themselves.
In 2000, physicians at Emory University set out to prove just how important clinicians’ personal and professional endorsements of nutrition are to their patients. To conduct this experiment, patients in a clinic waiting room viewed one of two similar videos of the same physician providing advice on nutrition and fitness. The only difference between the videos was that that in one, the clinician providing advice wore a bicycle helmet, placed an apple on her desk, and spoke for an additional thirty seconds about her own healthy habits, while these elements were absent in the other. Not surprisingly, the patients who viewed the former version deemed the physician healthier, more motivating, and more believable than the patients who viewed the latter video.[6]
Similarly, a 2009 study found that when a physician endorsed specific nutrition education materials during a visit, patients were much more likely to remember the materials, show them to others, and feel that the recommendations were specific to them as individuals, compared to controls who received the materials without any discussion during the visit (OR = 1.35, 95% CI = 1.00-1.84).[7] This was true when physicians made a point of endorsing other healthy lifestyle behaviors as well, including increasing exercise and quitting smoking. Another study showed that if a clinician weighed more than an overweight patient, he or she initiated a conversation about weight loss 11% of the time. However, if a clinician weighed less than an overweight patient, he or she discussed weight loss with the patient 89% of the time.[8] Thus, our habits matter to our patient, and if we practice what we preach, we can make a great impact on patients’ lives.
How can weight loss make a difference?
Multiple studies have measured the impact of small reductions in weight. Make your patients aware of the changes their body undergoes with weight loss. Below is a chart summarizing some of these changes.[9]
Table 2. Health benefits of a 10kg weight loss for those who are obese
Table 2. Health Benefits of a 10kg Weight Loss For Those Who Are Obese
Condition
Benefits
Mortality
20-25% fall in total mortality 30-40% fall in diabetes deaths 40-50% fall in obesity related cancer deaths
Blood Pressure
Fall of 10 mmHg systolic pressure Fall of 20 mmHg diastolic pressure
Lipids
Fall by 10% in total cholesterol Fall by 15% in “bad” cholesterol Fall by 30% in triglycerides Increase by 8% in “good” cholesterol
Angina
Reduced symptoms by 91% 33% increase in exercise tolerance
Diabetes
Fall of 30-50% in fasting blood glucose Reduces risk of developing diabetes by more than 50%
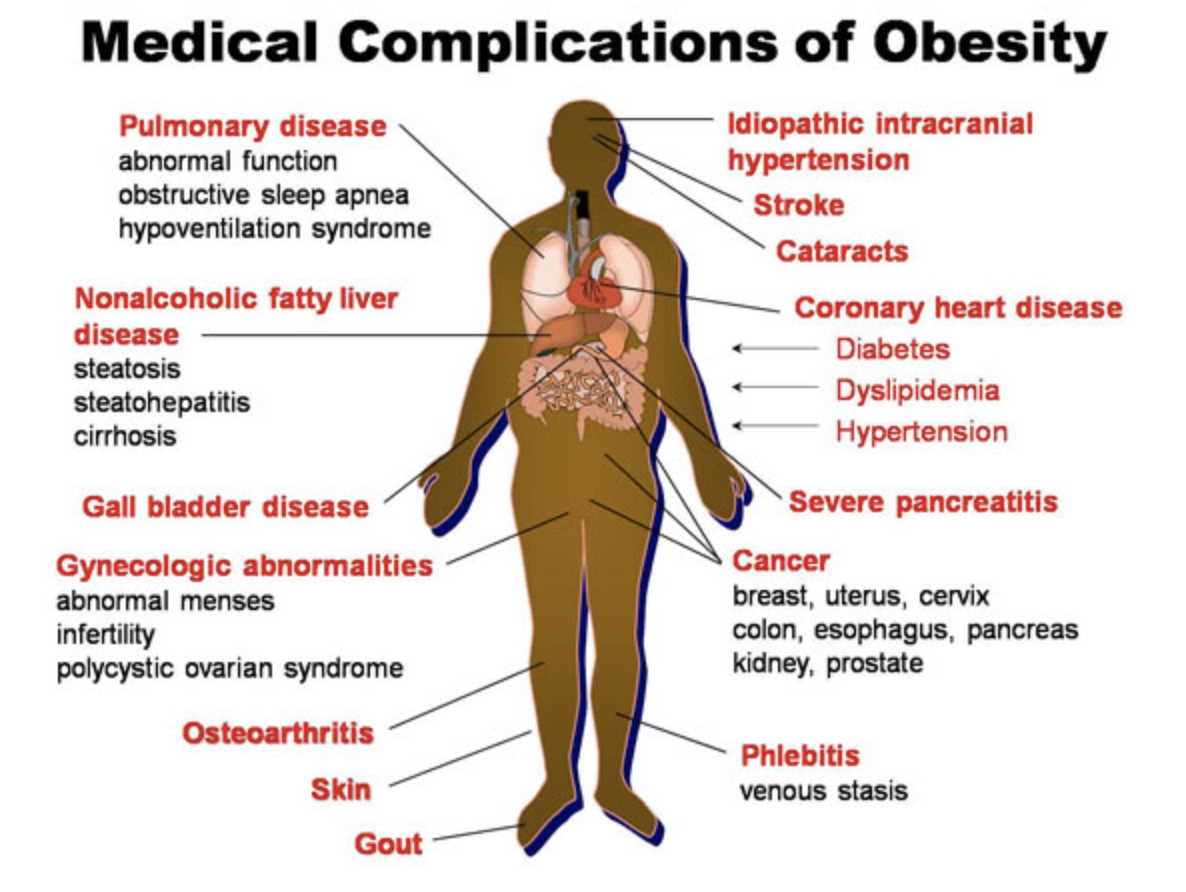
Highlight the number of medical conditions associated with obesity, but make sure to frame the discussion in a positive way. Explain that by losing weight, you can reduce your risk of developing many health problems. It is important to make it clear that a “normal” weight does not necessarily equate to having a healthy, nutrient-rich diet, nor does being obese necessarily mean a person lacks nutrients or eats unhealthy foods. Most dietitians agree that it is important to look beyond just numbers of calories. As with all aspects of Whole Health, explore this in greater depth on an individual basis.
Below is one image that illustrates the risk associated with obesity.’
Figure 2: Medical complications of obesity. Copyright pending. Image from: http://www.asyouage.com/19_Medical_Complications_of_Obesity.html
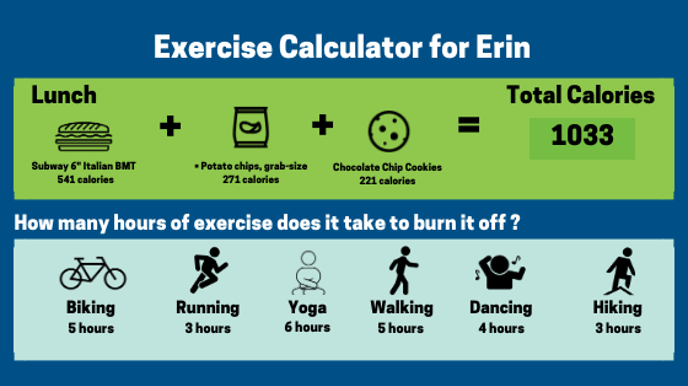
A common mistake that many of us make is to tell ourselves we can work off the calories we consume—that we can out-exercise a poor diet. While moving the body is an essential component of weight loss, exercise cannot make up for a lack of healthy nutrients in the diet. The impact of poor dietary choices on our weight is very difficult to overcome through exercise when not also combined with healthier eating. The image below derives from a calculator that determines how much exercise will burn off calories from a common fast food meal. For example, ordering an Italian sub sandwich from Subway, potato chips, and chocolate chip cookies, requires riding a bicycle for 5 hours, dancing for 5 hours, or running for 3 hours to burn the calories from that meal.
Figure 3. Calories burned through activities compared to calories ingested with fast food
Below are some resources to help patients calculate calorie intake:
Finally, emphasize that the patient’s weight is not a permanent state of being but constantly in flux, and the best way to stabilize this process is through achievable healthy habits. Use motivational interviewing techniques to encourage these habits.
Some basic nutrition guidelines
Whether you are discussing food and drinks with patients or thinking about your own dietary practices, the following 10 general guidelines can serve as a good starting point.
1. Tailor nutrition recommendationsto individual need, in the spirit of personalized, proactive, and patient-driven care. Collaborate with your patients to create an individualized food and drink plan that takes into account their economic resources, access to food, cooking ability, and religious and cultural factors. Explore these resources:
S. Department of Agriculture food pyramids for different ethnic and cultural groups.
2. Small changes in eating habits are typically easier to make than complete diet overhauls.[10] Clinicians should not feel like they are doing all the work; each individual should set goals, working with their clinician. These goals should feel realistic, and achieving one goal can often lead to the beginning of a cycle of setting and achieving other goals as well. If you are wondering what to change, review the components of the Standard American Diet, as listed above. Offer examples of possibilities, and encourage patients. For example, if they recognize that their soda consumption may be causing harm to their body, you might encourage them to decrease soda intake by a specified number of ounces per day. Similarly, if they do not want to completely remove burgers from their diet but are open to eating them less frequently, suggest that they only eat red meat once weekly.
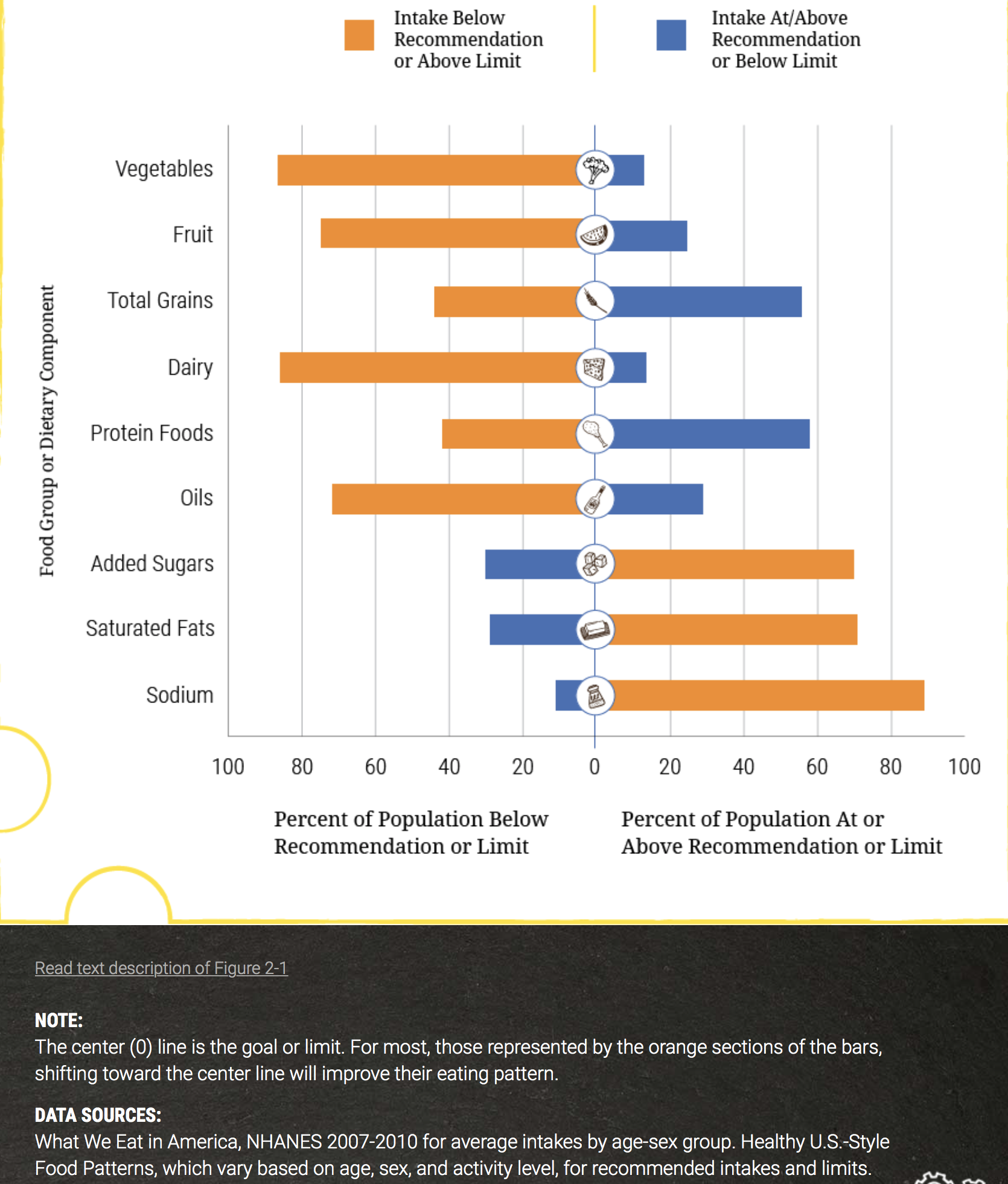
Meet each patient where they are at and help them set SMART goals (Specific, Measurable, Action Oriented, Realistic, and Timed).[11] See Figure 4 from the USDA 2015 Dietary Guidelines for Americans, which shows what percentage of Americans meet various dietary recommendations.
Figure 4. The Standard American Diet Versus the USDA Dietary Guidelines for Americans, 2015.[ref id=12] NOTE: The center (0) line is the goal or limit. For most, those represented by the orange sections of the bars shifting toward the center line will improve their eating paterns.
3. Which diet? You probably have been asked many times about which diet is the best one to follow. In general, research tells us that the diet that works best is whatever one a person is willing and able to stick with long-term.[13] Be familiar with the eating patterns recommended in popular diets (some of these are described below and in the “Choosing a Diet” Whole Health tool).
4. Meet nutritional needs through foods versus multivitamins or other dietary supplements.[14] Invest in healthy, nutrient-dense food. These foods have a high ratio of nutrient content relative to how many calories they contain. This is in contrast to energy-dense foods, in which the calories in the foods are way out of proportion to how nutritious they are. Certainly, it can be helpful to focus on a Mediterranean Diet,[15] or a whole foods, plant-based diet.[16] The 100 foods on the list of the World’s Healthiest Foods,[17] were chosen based on being not only nutrient-dense but also because they are familiar, tasty, and affordable. Many are also part of a Mediterranean diet. They are also whole foods; that is, they have not been extensively processed or modified from their natural state. Examples in different categories include (and most of these probably will not surprise you) the following:
Vegetables: asparagus, avocados, beets, bell peppers, broccoli, Brussels sprouts, cabbage, carrots, cauliflower, celery, corn, cucumbers, eggplant, fennel, garlic, green beans, green peas, greens (mustard and collard), kale, leeks, mushrooms (e.g., cremini and shiitake), olives, onions, potatoes, lettuce, sea vegetables, spinach, squash (summer and winter), sweet potatoes, Swiss chard, tomatoes, and turnip greens
Herbs and spices: basil, black pepper, chili pepper (dried), cilantro, coriander, cinnamon (ground), cloves, cumin, dill, ginger, mustard seeds, oregano, parsley, peppermint, rosemary, sage, thyme, and turmeric
The list is by no means all-inclusive, and these choices are always subjective to some extent, but it gives you some ideas. A simple food and drink suggestion for a Personal Health Plan (PHP) when you are pressed for time could easily be: “How about eating more of [insert one of the top 100 foods here]?” It is also entirely appropriate to use the elements of the Mediterranean diet, or other whole foods, plant-based diets to guide this sort of advice.
5. Dietitians, nutritionists, and health coaches are powerful allies in helping patients with their nutritional needs. Refer your patients to dietitians for a more in-depth discussion of dietary changes. Health coaches can help with goal setting and accountability, supporting people as they institute the goals they set for themselves with the help of clinicians.
6. Avoid oversimplifying. A common weight loss myth is that there are roughly 3,500 calories in a pound of body fat, and if you decrease caloric intake by 500 calories per day, you can lose one pound weekly. However, this figure is not accurate, and the weight loss equation is much more complicated than this.[18] Interestingly, the story of how we obtained “3,500” dates back to the work of a scientist named Bozenrad in 1911. He once measured 1 lb of human adipose tissue and found that it contained 87% lipid and 13% water. Another scientist named Wishnofsky expanded on his work in 1958 by using bomb calorimetry to measure 9.5 kcal in each gram of fat. Since there are 454 gm in 1 lb, and human adipose tissue in Bozenrad’s measurement was 87% lipid content, Wishnofsky determined that there are 395 gm of fat in 1 lb of fat tissue. He then rounded his original value of 9.5 kcal/gm to 9 kcal/gm and multiplied this by 395 gm to obtain 3,555 calories in a pound of fat.
Not surprisingly, the methodology behind this experiment is flawed. Ignoring rounding errors, Wishnofsky and Bozenrad analyzed only one sample, and subsequent studies have shown that the lipid content in a pound of fat varies significantly between people based on demographics and even within the same person at different phases of weight loss.
Two studies, entitled CALERIE 1 and CALERIE 2, found that we typically undergo two phases of metabolism during weight loss, and this affects how many calories we burn.[19,20] The first phase of weight loss lasts days to weeks and involves exhaustion of glycogen stores, small fat content, and water content. During this phase, lower calorie deficits are needed to achieve weight loss; participants 4 weeks into the study only needed to lose, on average, 2,208 calories per pound. Over time, as our glycogen pool is exhausted, our body begins breaking down protein and more fat content, and this leads to a slower second phase of metabolism. At this time, the body reduces thermogenesis. Study participants at 24 weeks, for example, needed to burn an average of 2,986 kcal/lb.
While it may not be beneficial to explain the details of the CALERIE studies to patients, it is important to avoid oversimplifying weight loss as a basic equation. Weight gain and loss are affected by many other factors, such as hormones, the microbiome, toxins, food sensitivities, stress, sleep, and many other factors. Moreover, it can be helpful to know that early gains from diet and exercise do slow down over time based on shifts in our metabolism, but patients should not be discouraged by this.
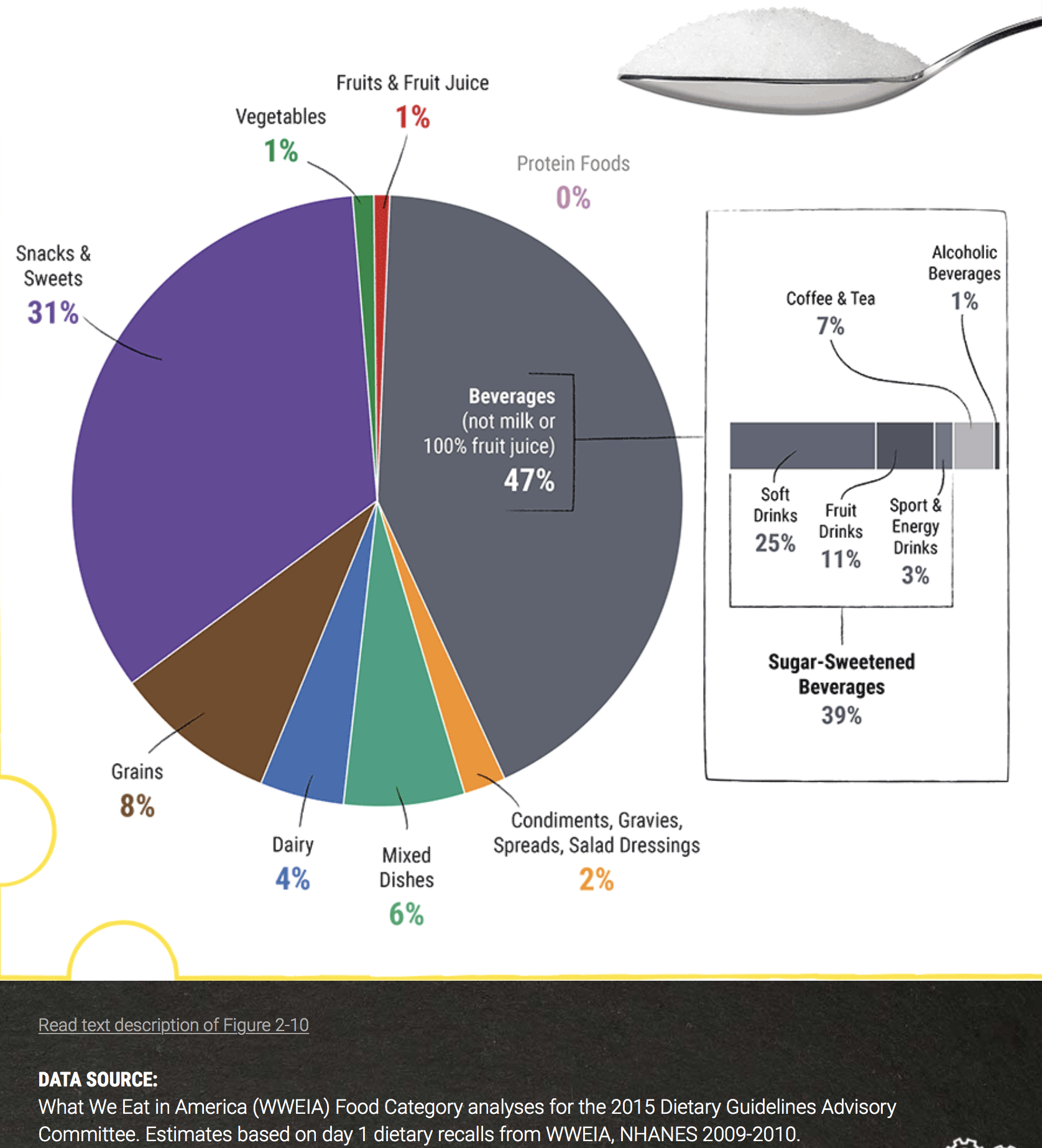
7. Choose beverages wisely. Around 21% of our daily caloric intake comes in liquid form. [21] Moreover, 47% of our dietary sugar intake comes from beverages (see Figure 5 below).
Figure 5: Dietary Intake of Sugar
If you are looking for one piece of advice to give patients who want to improve their nutrition, this may be it: changing what you drink has a powerful effect. Cut out or minimize intake of soda, sweetened tea or coffee, juice, alcohol, energy drinks, smoothies, soda or milk, and replace them with water. If patients miss the carbonated aspect of soda, consider carbonated water or kombucha. If patients miss the flavor of sweetened beverages, recommend naturally flavoring water with herbs and fruits (e.g., pineapple and mint-infused water). Total calorie intake (and proportion of healthy calories) are likely to decrease substantially, and overall health will likely improve.
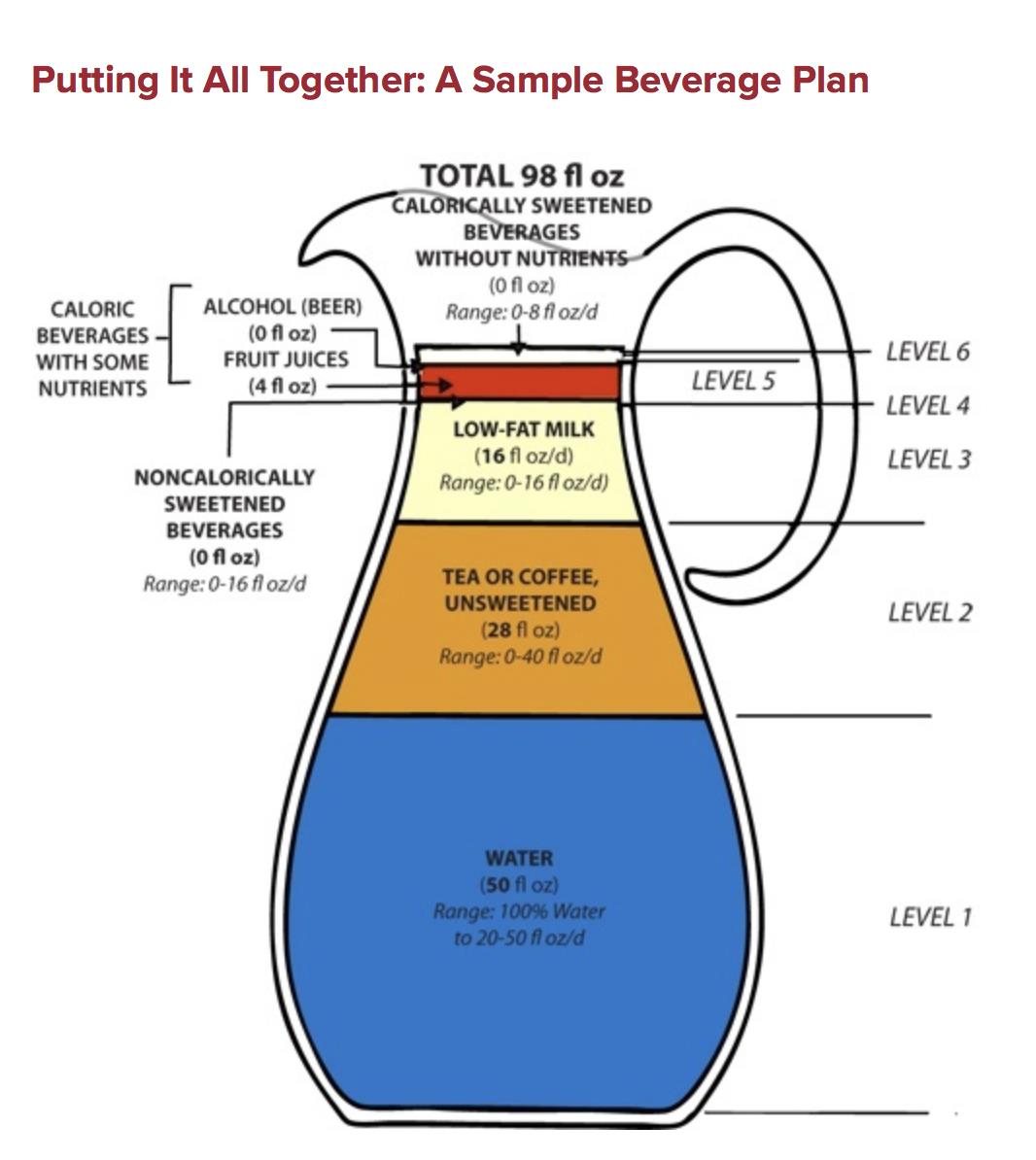
Alternatively, if patients are unwilling or unable to eliminate beverages other than water, consider creating a beverage plan for them with specific guidelines. See the sample beverage plan created by the Harvard School of Public Health, below.
Figure 6: Putting it All Together: A Sample Beverage Plan. Copyright pending. Source: https://www.hsph.harvard.edu/nutritionsource/healthy-drinks-full-story/ [ref id=22]
For more information on beverages, please refer to the “What We Drink” Whole Health tool.
8. Pay attention to portion sizes. How much of a food people actually eat may be much more than the serving size listed on the package. Many nutrition experts recommend getting 7-9 servings of fruits and vegetables daily. A serving is not as big as many people assume. For green leafy vegetables, such as spinach, kale, or lettuce, it is generally 1 cup. For other vegetables, a typical serving is 1/2 cup. A serving of fruit is 1/2 cup, which would equal a small banana, a slice of melon, or 1/4 cup of dried fruit. Fresh fruits and vegetables are best, but if these are not available or affordable, frozen is generally a better option than canned. Look for frozen or canned fruits without added sugars, and those packed in water or their own juice, instead of in syrup.
Keep in mind that it may be easier for people to meet recommendations than they might think. They can search online for photos of various serving sizes, go to ChooseMyPlate for a visual, and to Dietary Guidelines for Americans and more.
9. Share advice from people who have successfully made healthy behavior changes related to nutrition. For example, the national weight control registry recorded the habits of over 10,000 individuals who lost an average of 66 lbs and kept it off for 5.5 years. Here are four common themes from their experiences:
78% eat breakfast daily
75% weigh themselves at least once a week
62% watch less than 10 hours of TV per week
90% exercise, on average, about 1 hour per day
Visit the National Weight Control Registry for updates on research findings. While weight loss is just one aspect of a healthy approach to Food and Drink (and quality of food is a focus, not just quantity), this does speak to some overall recommendations for a healthy lifestyle.
10. Encourage mindful eating. It is easy to eat without even noticing what we are eating. Most of us have had an experience where the entire back of chips or bowl of popcorn seems to vanish, and we have no recollection of having eaten it. And, we may not eat because of physical hunger; it helps to notice how much of our eating is influenced by habit, emotion, social surroundings, and so on. We know that stress exposure alters the brain’s response to food in ways that predispose us to poor eating habits. [23]
Mindful eating involves recognizing when we are stressed and finding ways to counter these effects. As with all mindful awareness activities, it is not about judging so much as simply paying attention. Some suggestions that are widely used by instructors in mindful eating include the following:[24-26]
Focus on what sort of hunger you are experiencing. There is the actual physical state of hunger, but we may also eat because something has visual appeal, or because we like how it smells. We may eat for emotional reasons, because of a craving of some kind, out of habit, or for many other reasons.
Do not get too caught up in the “right” or “wrong” way you should eat, but simply note your level of awareness around experiencing food.
Recognize that each of us has unique experiences when it comes to eating. Get to know yours through paying attention, and then you will be more empowered to make choices about what and how you eat.
When you eat, do not do anything else. Do not watch TV or try to work. Focus on your meal (and perhaps the people with whom you are eating).
Periodically take time to note how hungry you are. Note how hungry you are before eating and then check in on your hunger as you eat. The goals is to stop eating if you are not experiencing hunger. Ideally, you can stop just before you are full, since it takes at least 20 minutes for your stomach to signal your brain that it is full.
Set your utensils down between bites.
Taste every bite. It can help to have a set number of times to chew for each bite you take. Start with 10-15 chews per bite.
Never eat while standing. Relax.
Note if there are other reasons why you are eating. Are you eating to satisfy hunger, or to fulfill an emotional need?
Consider taking a moment for gratitude or a pause after a meal (for satiation). Take time to focus on all the resources and people who made it possible for you to have what you are eating and drinking.
Use all your senses to guide your food choices.
For more information on mindful eating, refer to the “Mindful Eating” Whole Health tool and the “Mindful Awareness” Whole Health overview. Another excellent resource is the VHA National Center for Health Promotion & Disease Prevention’s “Mindful Eating Handout.”
Mindful Awareness Moment
Hunger
Take a moment, right now, to pause and check in with your body.
On a scale of 1 to 10, with 1 being “starving” and 10 being “overstuffed,” how hungry are you right now?
Where do you feel that hunger (or satiety) in your body? Is it in your stomach area, or somewhere else? What happens to your body when you become really hungry? Does it affect your mood, and if so, how?
As you make your way through this module, periodically check in and ask, “How hungry am I right now?”
What are the "right" things to eat?
Erin wants your advice regarding what to eat.
In general, it helps to think of nutrients in terms of two general categories:
Macronutrients are the energy-providing nutrients we need in large quantities: carbohydrates, fats, and proteins.
Micronutrients are the compounds we need in smaller quantities: vitamins, minerals, and phytonutrients.
This section reviews some important macro- and micronutrient tips you can incorporate into PHPs. After that is a discussion of other topics related to eating patterns, including the use of food pyramids, eating to reduce inflammation, and descriptions of some of the other popular diets that inspire patient questions.
Macronutrients: Some key recommendations you can make
One of the important ways to distinguish between different diets is by the proportions of macronutrients they recommend. For example, the Atkins diet promotes, especially in its first phase, very low carbohydrate intake. The South Beach diet focuses, in part, on “sensible” carbohydrates. You will learn more below about eating with close attention to glycemic index and load, which equates to consuming the “best” carbohydrates. And, of course, for better or worse, an entire branch of the food industry has sprung up since the last few decades because we have placed great value on eating low-fat foods
The 2015-2020 Dietary Guidelines suggests the following when it comes to macronutrients.[12]
“Choose a variety of nutrient-dense foods across and within all food groups in recommended amounts.”
Follow an eating pattern that is low in saturated fats, sodium, and added sugars.
Consume less than 10% of calories daily from added sugar.
Similarly, consume less than 10% of calories daily from saturated fats.
Keep sodium intake to less than 2,300 mg.
Mindful Awareness Moment
Your Own Diet
Take a moment to consider the quality of your own diet based on what you have eaten in the past week.
How many of the “World’s Healthiest Foods” have you eaten? How do you do with eating a Mediterranean diet, or a whole foods, plant-based eating pattern?
Did you eat vegetables daily?
How many servings of whole grains did you eat?
How many different colors of fruits and vegetables have you eaten?
The following sections will provide some specific suggestions about carbohydrates, fats, and proteins for you to incorporate into PHPs.
Carbohydrate tips
Most of the calories in the American diet come from carbohydrates. In plant-based foods, such as fruits, vegetables, grains, cereals, legumes, and beans, 90%-95% of the calories come from carbohydrates. Carbohydrates include the following:
Simple sugars such as fructose and glucose
Oligosaccharides including fructo-oligosaccharides (which are “food” for the good bacteria in our intestines)
Starches (which are energy storage molecules for plants)
Dietary fiber. Fiber is a carbohydrate, but our bodies cannot digest it. Fiber adds volume—but not calories—to food and it may increase satiety as well.
The United States Department of Agriculture (USDA) recommends that half of all grain intake come from whole grains. [27] In terms of how they affect satiety, carbohydrates fall between protein and fat, with protein being the most satiating of the three macronutrients. [28] Carbohydrates provide 4 kcal/gm in energy. This is roughly equal to the energy of protein, but less than fats, which contain 9 kcal/g. Consumption guidelines include the following recommendations.
Pay attention to fructose. Fructose is a simple sugar found in fruit, honey, and some vegetables. It is the sweetest of the simple sugars, and one form, high-fructose corn syrup (HFCS), is under considerable scrutiny these days. Fructose, on its own and in small quantities, may be a better carbohydrate choice than glucose in patients with prediabetes or diabetes due to its attenuating effects on blood sugar[29] (think of a serving of fruit, not a serving of juice drink, as the source). This is not true for high-fructose corn syrup, which typically is 50% fructose and 50% glucose, similar to sucrose or table sugar, which is not an ideal combination.[30]
Most Americans consume about 40 gm of fructose daily, mostly in the form of HFCS. Whether HFCS is worse than pure fructose or sucrose remains to be seen; evidence is conflicting. We do know that fructose consumption from processed foods has significant effects on, for example, all the components of metabolic syndrome.[31] (For more information, refer to the “Endocrine Health” Whole Health overview, and the “Hypertension” and “Lipids,” Whole Health tools; these topics are the main components of metabolic syndrome.) It is important to keep in mind that fruit is an important source of fructose (hence the similarity in their names), but the fructose in fruit—even though it may be in higher quantities—is accompanied by fiber, which is known to attenuate rises in blood sugar. In contrast, HFCS is rarely consumed with fiber. In fact, it is often consumed as a carbohydrate in isolation; for instance, it is practically the only ingredient in soda and other sugar-sweetened beverages.
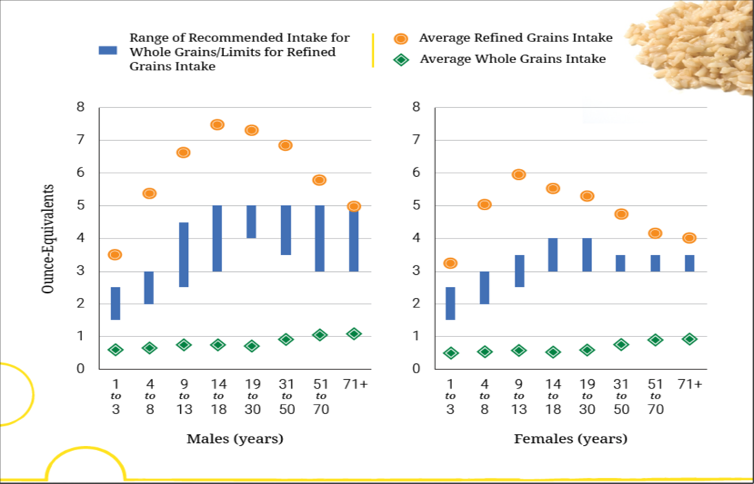
Do not get too bogged down in simple versus complex carbohydrates. It is frequently suggested that complex carbohydrates are better than simple ones. Many experts tell patients to eat complex carbohydrates, because they believe they are better for overall health. By definition, simple carbohydrates are composed of mono- or disaccharides (they have just one or two sugar molecule groups in them). Complex carbohydrates are polysaccharides (they have many simple molecules linked up). In short, whether or not carbohydrates are simple or complex is less important than focusing on which foods the carbohydrates come from. It is best to advise patients to eat whole grains and products made from them, as well as fruits, vegetables, and legumes, while minimizing foods with made with sugar or refined white flour. This is especially important because most Americans do not eat enough whole grains (see figure below).
Figure 7. Recommended Grain Intake Note: Recommended daily intake of whole grains is to be at least half of total grain consumption, and the limit for refined grain is to be no more than half of the total grain consumption. The blue vertical bars on this graph represent one half of the total grain recommendations for each age-sex group, and therefore indicate recommendations for the minimum amounts to consume of whole grains or maximum amounts of refined grains. To meet recommendations, whole grain intake should be within or above the blue bars and refined grain intake within or below the bars.
Choose carbohydrates based on glycemic index and glycemic load.Rather than focusing on whether a carbohydrate is simple or complex, it may be more helpful to choose which carbohydrates to eat based on how they are metabolized. Glycemic index and glycemic load take into account how much a given food raises blood sugar levels. Glycemic index (GI) compares how much a particular food that contains 50gm of carbohydrates will raise blood glucose levels 2 hours after eating, relative to an equivalent amount of glucose (or white bread). The problem with the GI is that different foods have different amounts of carbohydrate by weight. For example, in order to get 50 gm of carbohydrates from carrots, you would have to eat at least 5 cups of them. To allow for more realistic comparisons, glycemic load (GL) is used instead. Glycemic loads are like GIs, but they account for serving size.[32] GL is ultimately the GI multiplied by the amount of carbohydrate per serving of a given food. For more information, please refer to the “Glycemic Index” Whole Health tool.
High glycemic index and load are clearly associated with increased risk of type 2 diabetes. In a 2014 pooled study that included 3.8 million person-years of follow- up, the quintile of patients with the highest food measures of GI and GL had a 33% higher risk of developing the disease.[33] There is also a correlation between high-GL diet and ischemic (but not hemorrhagic) stroke risk,[34] obesity,[35] and chronic inflammation.[36] A 2008 meta-analysis found that high GI and GL diets correlated with higher risks of certain cancers, including colon and ovarian cancer (but not pancreatic or breast cancers).[37] A low GI/GL diet also reduces gallbladder and coronary artery disease risk.[38]
An interesting area of recent research on glucose tolerance is the “second meal effect.” If you eat a low GI/GL breakfast, your blood sugar will not climb as high after eating lunch. The same thing occurs after you eat a low GI/GL dinner; your blood sugar will not be as high at breakfast the next morning.[39,40] It is in part because of the second meal effect that people with diabetes are encouraged to eat fewer small meals during the day. Carbohydrates are absorbed more slowly and sugars stay lower on average if multiple small meals are eaten, rather than just a few large ones.[41]
Avoid refined carbohydrates. Because of their high glycemic load, cutting refined carbohydrates out of your diet can sometimes result in dramatic improvements in health. Common refined carbohydrates include the following:
Corn chips
Potato chips
Pizza crusts
Most flours
Pastries
Cookies
Biscuits
White rice
Pasta
Pies
Bagels
Bread
Buns
Muffins
Sugar
Soda
Breadcrumbs
Cereal bars
Granola
Toffee
For a more comprehensive list, go to the Diagnosis Diet website.
Eat your fiber. The metabolic fate of carbohydrates is determined largely by the company they keep. Fiber, which is composed of carbohydrates the body cannot digest, influences carbohydrate absorption in the gut, decreasing the rise in blood levels of glucose, insulin, and lipids that normally occurs after eating.[42-44] There are two main kinds of fiber. Soluble fiber has beneficial effects on absorption of glucose, insulin, and lipids. Insoluble fiber acts as a laxative and bulking agent. Few Americans consume the recommended daily intake of fiber, which is 14 gm/1,000 kcal, or roughly 25 gm for women and 38 gm for men. Some argue that fiber intake should perhaps be as high as 50 gm a day for those with diabetes.[45] Because fiber has important health benefits but is often neglected in the American diet, a discussion about fiber can be another potentially good starting point for the “Food and Drink” section of a PHP. High fiber intake significantly improves health. Fiber intake is associated with reduced all-cause mortality after myocardial infarction.[46] Intake is inversely associated with esophageal cancer incidence,[47] stroke risk,[48] and cardiovascular disease.[49] Fiber should be used with caution in people with functional bowel problems, such as irritable bowel syndrome, because it can exacerbate bloating, constipation, and diarrhea.[50]
When checking nutrition labels, aim for foods with a favorable sugar-to-fiber ratio. This means that there should be no more than five times as much sugar as there is fiber. Avoid foods with higher sugar-to-fiber ratios.
The types of fats you eat make a difference. For quite some time (roughly 1980-2015, in terms of Dietary Guidelines for Americans), the popular belief was that fats are “bad” for us in any form. Fat-free foods have been touted commercially as the solution to all our nutritional ills. However, fat-free eating requires that the calories be replaced with calories in another form. If this “other form” is carbohydrates, eating them may not be as helpful as we assume.[51] When large quantities of carbohydrates are eaten, those that are unneeded are stored as fat.
In excess, certain types of fats can contribute to health problems, but they are essential to healthy functioning, providing us the necessary building blocks for cell membranes, myelin sheaths around nerves, and steroid hormones. Fats are also essential for absorption of the fat-soluble vitamins, A, D, E, and K. Many people’s bodies are genetically programmed to hold on to fat; for our ancestors, this could be an advantage during times when food was scarce.
There are a few main categories of fats,[52] and knowing more about them can help patients make good food choices:
Saturated fats (SFAs) are those without any double bonds in their carbon chain. They are solid at room temperature and include animal fat, butterfat, coconut oil, palm oil, and kernel oils. Most experts recommend keeping saturated fat intake to a minimum.
Monounsaturated fats (MUFAs) are liquid at room temperature and found in avocado, peanut, olive, and canola oils. They have one double bond in their carbon chain.
Polyunsaturated fatty acids (PUFAs) are also liquid at room temperature. They have more than one double bond and include fish, sesame, sunflower, walnut and corn oils. The PUFAs linoleic acid (LA) and alpha-linolenic acid (ALA) are essential; that is, they are necessary but the body cannot synthesize them and therefore they must be obtained through the diet.
Essential PUFAs are in vegetables such as dark, leafy greens and purslane. They also come from animals that consumed LA- or ALA-rich algae and plant foods.
Omega-6 fatty acids have a double bond at position 6 of their carbon chain. They play an important role in inflammation. Inflammation is important to an organism’s survival, but chronic inflammation can be harmful. Omega-6s rev up the chemical reactions that we normally attempt to suppress with medications such as nonsteroidal anti-inflammatories. Linoleic acid is an omega-6 fat, which is plentiful in most diets. It is in many nuts and seeds and in the fat of some animals, like pigs. Red meats and other animal products lead to creation of proportionally more omega-6 fatty acids than other foods.
Omega-3 fatty acids have a double bond at position 3 in their carbon chain. They contribute to the reduction of inflammation, based on how they influence various chemical pathways in the body. The most important omega-3s to know about are docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). Omega-3s are not commonly consumed as part of the standard American diet. They are in fish, as well as walnuts, leafy greens, and many seeds.
The essential omega-3, ALA, is found in walnuts, flaxseeds, chia seeds, hemp seeds, pumpkin seeds, and canola oil. It can be metabolized to DHA and EPA, but the process by which humans convert ALA to DHA and EPA is inefficient; therefore, it is best to get DHA and EPA directly from the diet, rather than relying on conversion of ALA.
DHA and EPA are found mainly in fatty, deep-sea fish, krill, and algae. The acronym SMASH can help patients remember fish that are good sources of DHA and EPA: salmon, mackerel, anchovies, sardines, and h
Trans-fats replace the cis-double bonds in MUFAs and PUFAs with trans– bonds. Found in processed food sources,[53] trans-fats were created to allow foods to have a longer shelf life. Unfortunately, they may decrease the duration of human life, because they are known to increase cholesterol levels and coronary artery disease.[54,55] It is best to avoid all foods made with trans-fats and partially hydrogenated oils of any kind. The United States now bans use of trans-fats in all foods offered in restaurants and grocery stores.
Ensure you get enough omega-3s.The essential PUFAs are precursors to prostaglandins, leukotrienes, and other compounds that control levels of inflammation in the body. With the increased consumption of highly processed foods, the ratio of proinflammatory omega-6 fats to anti-inflammatory omega-3 fats in the diet has steadily increased, increasing the number of people whose bodies are in a state of chronic inflammation. Current ratios of omega-6s to omega-3s range from 15:1 to 25:1. The ideal ratio is the subject of some debate, but most sources suggest it should be more in the 2:1 or 4:1[56] Inflammation has an important physiological role, but a system of checks and balances is needed; many of today’s chronic diseases are associated in some way with chronic inflammation.[57] It is worth discussing whether or not to recommend omega-3 supplements for many patients.
Note: Please refer to the Passport to Whole Health, Chapter 15 on Dietary Supplements for more information about how to determine whether or not a specific supplement is appropriate for a given individual. Supplements are not regulated with the same degree of oversight as medications, and it is important that clinicians keep this in mind. Products vary greatly in terms of accuracy of labeling, presence of adulterants, and the legitimacy of claims made by the manufacturer.
Eat to improve your cholesterol panel. Many people have abnormal lipid panels and struggle to improve them. A few general points to consider include the following:
Triglyceride levels increase primarily due to eating foods with a high GI; that is, they are closely linked to carbohydrate intake. People with diabetes and/or thyroid disorders often have elevated triglycerides.[58,59]
High-density lipoproteins (HDLs) transport excess triglycerides and cholesterol back to the liver from outlying cells, and low-density lipoproteins do the reverse. For this reason, HDL often is labeled “good cholesterol,” and LDL labeled as “bad.”
Foods that raise LDL cholesterol levels most are: (1) those high in saturated fats, and (2) those with a high GI. These foods have a much more significant impact than foods that are high in dietary cholesterol, such as eggs, shrimp, shellfish, and caviar.
For more information, refer to the “Lipids” Whole Health tool.
Guidance with eating protein
Get enough protein (but not too much) each day, from healthy sources. Adults are encouraged to obtain 10%-35% of their daily calories from protein. That equates to 56 gm for men and 46 gm for women.[60] Eating 2-3 servings of protein-rich foods a day seems to cover needs. Examples of protein serving include[60] the following:
A 3-oz piece of meat, which has about 21 gm of protein; a typical 8-oz serving has over 50 gm
8 oz of yogurt, which has about 11 gm, or 8 oz of milk with 8 gm
One cup of cooked beans contains roughly 16 gm of proteins.
Animal protein is a source of significant amounts of protein. However, many meats contain a fair amount of saturated fat and are sources of trimethylamine N-Oxide (especially for red meats and processed meats), which increases risk for cardiovascular events and cancer; they are best eaten with less frequency. Calorie for calorie, protein is the most satiating or filling of the macronutrients.[61] The average American consumes roughly 100 gm of protein daily, despite the fact that recommendations encourage a lower quantity.[62] A diet high in animal protein can be taxing for the liver and kidneys.
Eat all of your essential amino acids. There are certain amino acids that must come from the diet; our bodies cannot synthesize them. These amino acids have critical antioxidant and anti-inflammatory properties and are key chemical ingredients for many of the body’s chemical reactions. It helps to vary protein sources in your diet. Bring in meat, fish, legumes (beans, lentils), eggs, nuts, seeds, and whole grains such as quinoa to add variety.
Vegetarians can get the full spectrum of amino acids in the diet if they eat a variety of the foods listed above. Bacteria that live in our digestive tract also serve as a protein source. Epidemiologic studies show that those who eat a nutritious, primarily vegetarian diet derive health benefits from doing so.[63] Of course, “vegetarian” is not synonymous with “healthy.” A diet of sports drinks and corn chips may even be vegan, but it is not nutritious.
Micronutrients: vitamins and minerals
Micronutrients are essential for life. They serve many vital roles in our health and development including production of adenosine triphosphate (ATP), hormones, enzymes, and neurotransmitters. The multitude of biochemical reactions that happen throughout the body require micronutrients as cofactors. They include vitamins and minerals, as well as phytonutrients. One can become deficient in micronutrients in the absence of a well-balanced diet. Specific clinical findings related to various deficiencies, while beyond the scope of this overview, are available at the Public Health Reviews.[64]
Eat your vitamins. Vitamins were discovered in the early 1900s and were originally called “vital amines” because it was initially thought that they all contained amino (nitrogen) compounds.[65] The name was changed to “vitamins” after it was discovered this wasn’t true. Vitamins are classified as water-soluble (B vitamins, vitamin C) and fat-soluble (vitamins A, D, E, and K). Many people follow the recommended dietary allowance (RDA) created by the Institute of Medicine to ensure they are consuming the necessary amounts of vitamins each day. However, the RDA focuses on the minimum amount of vitamins required to prevent deficiency. Dietary Reference Intake (DRI) is probably a more reliable number to follow, if possible. The DRI of a given micronutrient depends on many things such as sex, age, overall health status, and, for women, whether or not they are pregnant or lactating.
Most people can get all of the vitamins they need through a balanced diet (this is difficult with vitamin D, however). Vitamin B12 is the only vitamin that is available solely through animal sources, putting vegans at risk for deficiency; for this reason, vegans should always be asked about B12 supplementation. If people have a very poor diet (e.g., they live in an urban “food desert”) or they absolutely insist on taking a multivitamin supplement, it is important to be able to offer good advice on how to select an appropriate one.
Eat your minerals, too. There are approximately 18 minerals necessary for our physiologic functioning. Table 3 briefly summarizes information about several of the minerals that are most likely to be discussed in a clinic visit—iron, calcium, zinc, selenium, and magnesium. In general, these are available on the VA formulary.
Table 3. Micronutrients: Functions, Sources, and Clinical Tips[66-68]
Micronutrient
Main Function
Comments
Iron
Part of hemoglobin and myoglobin Necessary for red blood cell development Aids with immune function
Found in meat, and is more absorbable in this form, called heme iron Plant sources (non-heme iron) include beans, spinach and other leafy greens, brewer’s yeast, pumpkin seeds, blackstrap molasses, sunflower seeds, almonds, and raisins
Bioavailability of non-heme iron is increased when consumed with vitamin C Can increase daily intake by cooking with non-coated iron pans
If taking an iron sulfate supplement and constipation is a problem, try using a chelated iron (e.g., iron bisglycinate)
Calcium
99% of body calcium is in bones and teeth
Dairy is a major food source Nondairy sources include dark leafy greens (collards, mustard greens, turnip greens, bok choy), sesame seeds, tahini, almonds, soybeans, tofu, and garbanzo beans
The rest is used for muscle contractions, nervous system function, and blood clotting
Sardines and mackerel (canned with bones), salmon with bones, and raw oysters also have it as do fortified fruit juices and soy milk
Mean intake ranges from 870-1,270 mg daily for men and 750 -970 mg daily for women.[69,70]
Ethanol, caffeine, and fiber can increase fecal excretion[71]
If not, taking a supplement with added vitamin D can be helpful to bring levels up to the DRI.*
Aspartame, glucose, excess sodium, and excess protein increase urinary excretion Recent trials indicate that calcium levels
Recent trials indicate that calcium levels may modestly negatively influence cardiovascular risk and must be considered in advising patients.[72]
Note that a 2014 prospective cohort study of data from the Nurses’ Health Study (n=74,245) did not find a link between calcium supplement intake and cardiovascular risk in women.[73]
Zinc
Critical to immune function, wound healing, and prostate health
Sources include oysters, beef, pork, chicken, and egg yolk. Also found in legumes, nuts, seeds, and whole grains
Consider if symptoms of poor wound healing, frequent infections, inflammatory bowel disease (IBD), acne, or psoriasis exist
If taking more than 30 mg daily, it is suggested to take zinc with a supplement that contains copper as well, as zinc and copper compete for absorption in the small intestine
Most experts recommend 8 mg daily for females and 11 mg daily for males
Selenium
Antioxidant that works with vitamin E Important for thyroid and immune
Found in seafood, meats, legumes, and whole grains, but also specifically in Brazil nuts.
Eating two nuts daily is sufficient to maintain healthy selenium levels. The levels of selenium in nuts and grains depends on the levels of selenium found in the soil.
A Cochrane review of selenium and cancer prevention showed that those in the highest quartile of selenium intake compared to those in the lowest quartile of selenium intake had 31% lower cancer risk and 45% lower cancer mortality risk as well as a 33% lower risk of bladder cancer and, in men, 22% lower risk of prostate cancer.[74]
Magnesium
Cofactor for over 300 different enzymatic reactions
Found in large amounts in green vegetables, but can also be found in whole grains, nuts, legumes, meat, fish, and dairy
Necessary for muscles and blood vessels, protein and fat synthesis, energy production, and the synthesis of urea
In supplement form, magnesium citrate and magnesium glycinate are the most absorbable forms.
Inadequate magnesium intake is common in the United States h
Toxicity may develop in patients taking high doses of magnesium-containing antacids and laxatives. The first sign of magnesium toxicity is diarrhea.
The maximum recommended amount of magnesium is 1,000 mg per day before patients develop symptoms of toxicity.
Can be taken to help patients with constipation, muscle cramps, headaches, anxiety, depression, kidney stones, and diabetes. It may also be helpful for patients with hypertension[75]
* DRI = dietary reference intakes
Keep sodium (salt) and potassium balanced
In terms of electrolytes, potassium is mostly intracellular, and sodium and chloride (the electrolytes in table salt) are mostly extracellular. Sodium deficiency is rarely a problem in the United States, given that so much of our food is processed, pre-seasoned, and over-salted, but it can occur with starvation, diarrhea, or vomiting. Most Americans exceed the tolerable upper intake level for sodium, with an average intake of 5-6 gm/day.[76] For more information on how to eat less sodium refer to, “The DASH Diet” Whole Health tool in the “Digestive Health” Whole Health overview. For more information on salt, refer to the USDA handout on salt and sodium, and several VA Nutrition and Food Services handouts on lowering sodium intake. Consider having people replace table salt with health-promoting spices, such as turmeric. For ideas, share the MOVE! patient education handout, “Spice It Up.”
Potassium, in contrast to sodium, often is depleted. Depletion may be due to medications or for other reasons. Potassium is important for nerve transmission, muscle contraction, glycogen and glucose metabolism, and cellular integrity. Potassium is found in potatoes with skin, tomatoes, bananas, dairy, legumes, seafood, broccoli, almonds, raisins, and peanuts. Potassium deficiency can occur with diarrhea, vomiting, starvation, taking certain diuretics, and magnesium deficiency. Of course, it is important to remember that that for certain medical conditions (e.g., chronic kidney disease) there may be dietary restrictions for potassium. “Dietary Guidelines” offers more information on the potassium content of foods.
Food Pyramids as a Nutritional Tool?
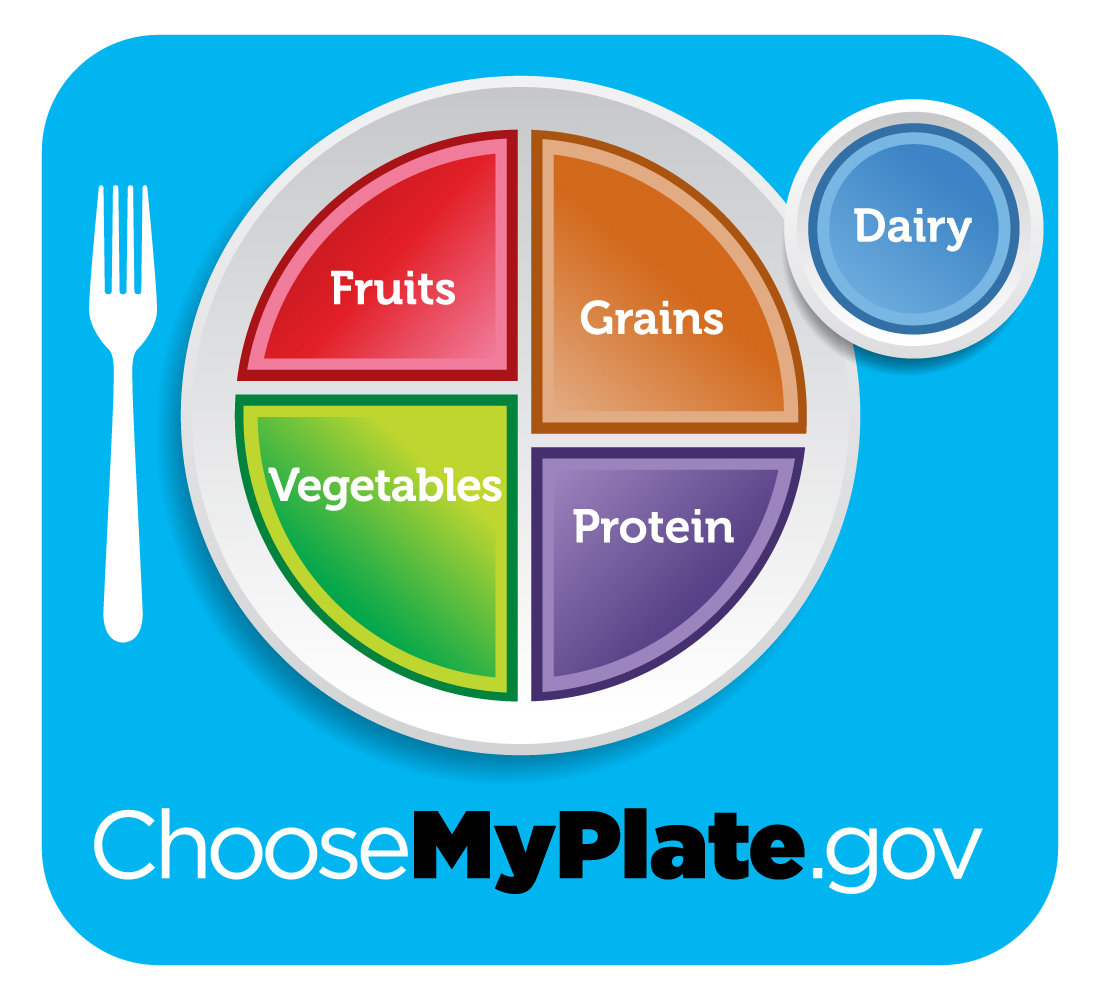
After its creation in 1992, many people used the USDA Food Guide Pyramid as a guide for how to eat. Its emphasis on breads and cereals at the base of the pyramid may not have been ideal. As additional nutrition research was done, portions and portion sizes became the focus of federal nutrition guidelines. “Choose My Plate,” the USDA’s most recent guidance related to portion size, was introduced in 2010 and has replaced the USDA Food Pyramid.[77] It shows a plate divided into four unequal sections, with vegetables and fruits together making up half the plate. Grains and protein make up the other half. (See Figure 8.) A circle representing dairy is off to the side. In Choose My Plate, grains are divided into two subgroups: whole grains and refined grains; the recommendation is that half of the grains a person eats should be whole grains.[78] Visit ChooseMyPlate for more information about using this nutrition tool.
Figure 8. Choose My Plate. [ref id=79] http://www.choosemyplate.gov
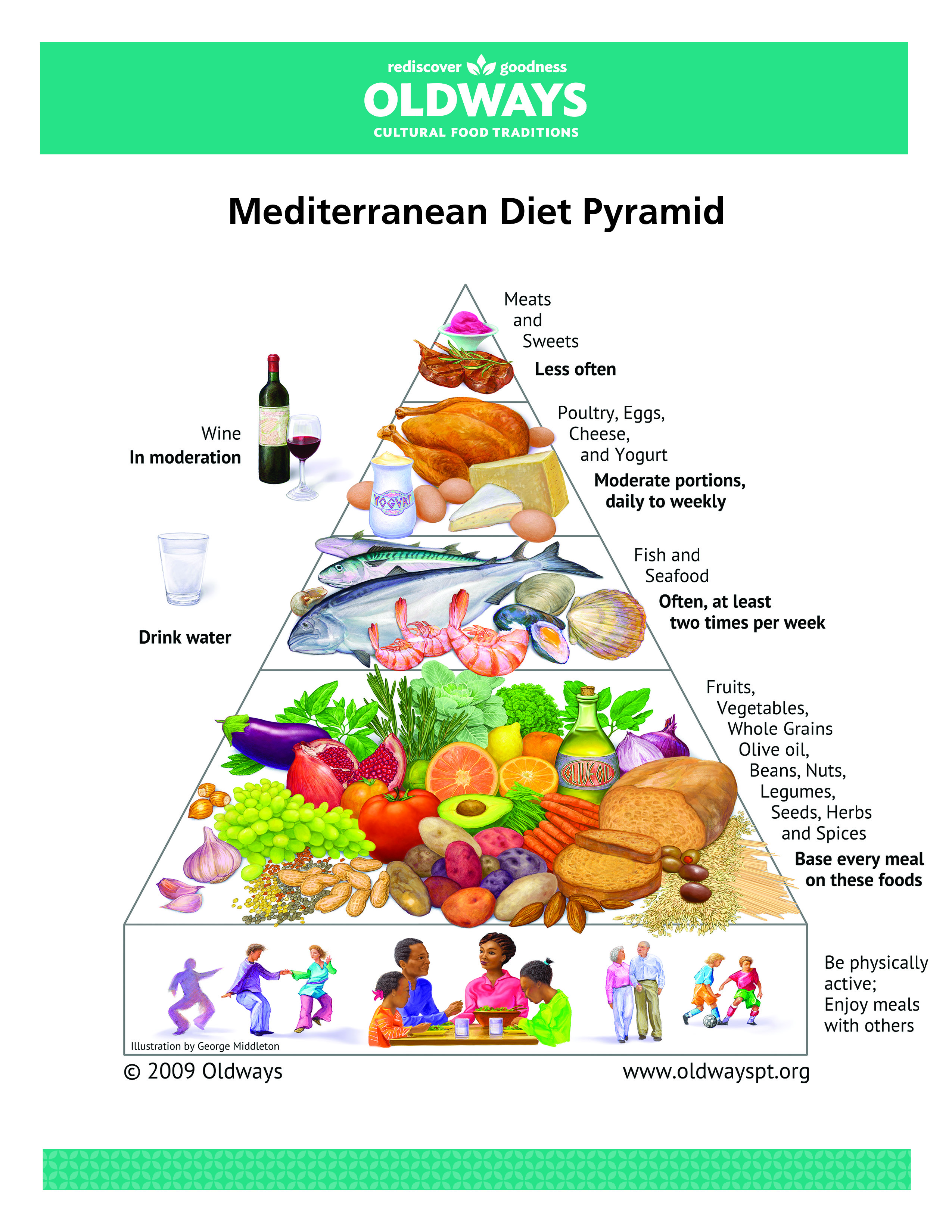
A number of other food pyramids have been created over the years, including the University of Michigan’s Healing Foods Pyramid that emphasizes plant-based choices, variety, and balance. Many dietitians recommend focusing primarily on Dietary Guidelines and ChooseMyPlate when providing specific recommendations for patients, vs. using food pyramids. The Mediterranean diet food pyramid is still used with some frequency in research. It is featured in Figure 9.
Figure 9. Oldways Health Through Heritage Mediterranean Diet. Reprinted with Permission from Oldways, https://oldwayspt.org/resources/oldways-mediterranean-diet-pyramid.[ref id=80]
Different Food Plans
What follows are tips about choosing the right overall eating approach or plan. While some of the eating plans mentioned below are popularly referred to as “diets,” it may be best not to overuse that term, given the negative connotation the word can have for many people.
Consider eating organic, but focus on foods that matter most
Organic foods are farmed without synthetic pesticides or fertilizers, and are processed without industrial solvents, irradiation, or food additives. Early research showed that organic food is not necessarily safer than food grown through conventional agricultural practices (conventionally grown food is already considered safe by USDA practices). [81] But, more recent studies have demonstrated benefits, including decreased risk of cancer.[82] The Environmental Working Group has created two lists, referred to as the Dirty Dozen™ and the Clean 15™.[83] These lists highlight which 12 fruits and vegetables are the most pesticide-laden after cleaning, and which 15 are the least.
Copyright Environmental Working Group, www.ewg.org. Reproduced with permission
For more information, refer to the “Food Safety” Whole Health tool.
Know about different food plans
Each year, new popular diets emerge, and patients often have questions about them. Below is some general information about several of the most important diets to know. Refer to the “Choosing a Diet” Whole Health tool, for more detailed information.
Anti-Inflammatory Diet
Chronic inflammation is linked to a number of diseases, including cancer, asthma, chronic pain, cardiovascular disease, and diabetes. It is possible to modify what a person eats so that inflammation becomes less likely. An anti-inflammatory diet emphasizes nutrient dense, whole foods that contain antioxidants and other compounds that diminish, or at a minimum, do not contribute to, inflammation in the body. Like other healthy diets, the anti-inflammatory diet emphasizes whole and minimally processed foods, including vegetables, fruits, healthy fats (particularly omega-3 fats), whole grains, and herbs and spices. Consumption of proinflammatory foods such as red meats, highly processed foods, and dairy fats is reduced. Evidence suggests that an anti-inflammatory diet reduces cancer,[84] cardiovascular disease,[85] and asthma.[86] Studies also show benefits for chronic pain,[87] inflammatory bowel disease,[88] and osteoporosis.[89] Future research is expected to show benefit in the setting of other autoimmune diseases as well. Refer to “Choosing a Diet” Whole Health tool for more information.
Summary: This diet is a useful adjunct treatment for chronic diseases, but also can serve as a general dietary recommendation due to reduction in cancer and cardiovascular risk.
Elimination Diet
Elimination diets involve removing particular foods or food groups for a set period of time, usually 2-3 weeks, and then reintroducing these foods systematically to see if they provoke symptoms. Usually one new food is added back in every three days to see if it triggers symptoms. This information helps create a new eating pattern. There has been positive research for the elimination diet for rheumatoid arthritis,[90] irritable bowel syndrome (IBS),[91] migraines,[92] atopic dermatitis,[93] ADHD,[94] and other diagnoses. For more information, refer to the “Elimination Diets” tool.
Summary: This diet can be used to treat specific chronic diseases, especially when triggers are unknown.
Mediterranean Diet
The Mediterranean diet follows traditional eating patterns from countries surrounding the Mediterranean Sea. It emphasizes fruits, vegetables, legumes, and whole grains. Dairy and meats are limited, with most animal protein coming from fish. Olive oil is used for cooking. An important aspect of the Mediterranean approach to eating is enjoying meals in the company of others. When compared to low-fat diets, Mediterranean diets are more effective in sustaining long-term improvements in inflammatory markers and cardiovascular risk factors like blood pressure and obesity.[95,96] Further studies have shown similar outcomes, including improved fasting glucose and markers for metabolic syndrome. [97] The Mediterranean diet is also linked to a lower risk of many cancers,[98] as well as benefits to cognition in older adults.[99] It also is associated with reduced telomere shortening, which suggests that it can increase longevity.[100]
Summary: This diet may be the best-studied diet for overall longevity and reduction of chronic disease. Like the anti-inflammatory diet, it has been studied for specific diagnoses. Overall, the diet is very similar to the anti-inflammatory diet.
Paleolithic nutrition
Paleolithic nutrition (and related diets, such as “The Paleo Diet”) are designed to be similar to the diet of our hunter-gatherer ancestors, with the logic that our genes are evolutionarily adapted to this diet.[101]Overall, this eating pattern allows more animal protein than the Mediterranean diet, in the form of lean meats, but it also emphasizes fruits, non-starchy vegetables, fish, nuts, and seeds. The diet discourages eating grain, dairy, legumes, processed foods, refined oils, and sugars. However, eating in this fashion might be challenging.[102] Modern animals are significantly different than their Paleolithic ancestors (notably, more plump). Vegetables were smaller and less palatable until farming during the Neolithic period, and grains, such as corn, were wild grasses with tough kernels. The average lifespan was less than 30, so it is not clear that the diet promoted longevity.
More research is needed, but this style of eating may be helpful in preventing problems related to metabolic syndrome.[103,104]
Summary: Positive aspects of this diet include a focus on fruits and vegetables and avoidance of processed foods. However, more research is needed, and it is important not to be caught up in the assertions made by commercial interests that tout “Paleo” eating.
Vegetarian/vegan diets
Vegetarians do not eat meat, fish, or poultry. Vegans also avoid all other animal products such as dairy, eggs, and honey. People become vegetarian or vegan for health, environmental, economic, or ethical concerns. A well-balanced vegetarian diet meets all known nutrient needs (including daily protein intake).[105] Studies have found that vegetarians have decreased incidence of cardiac disease,[106] and vegans with type 2 diabetes have better glycemic control than those who eat meat.[107]. Research also supports a vegetarian or vegan diet for weight loss,[108] reduction of systolic and diastolic blood pressure,[12] and prevention and treatment of diabetes.[109] A small study also reported improvements in neuropathic pain in subjects with type 2 diabetes following a vegan diet.[110]. One common nutritional deficiency among vegetarians, and vegans in particular, is vitamin B12. Vegans can either take supplemental Vitamin B12 or cook with nutritional yeast, which is rich in B12. Other deficiencies to look out for in this population include zinc and iron.
Summary: Both vegetarian and vegan diets prevent cardiac and metabolic disease and can result in weight loss. If balanced and low in processed foods, a vegetarian and vegan diet can meet all of a patient’s nutritional needs.
DASH Diet
DASH stands for Dietary Approaches to Stop Hypertension. It was initially recommended for those with hypertension or at risk for it, but subsequent studies have found that this diet is also helpful for improving cholesterol levels and insulin sensitivity.[67] The diet encourages high intake of fruits, vegetables, whole grains, and low-fat dairy. Fish, poultry, legumes, nuts, and seeds are also included, while red meats, saturated fats, and sweets are limited. In hypertensive patients, following the DASH diet resulted in a drop in systolic pressure of 11.6 mm Hg and a drop in diastolic pressure of 5.8 mm Hg.[67]
Summary: This diet shares many of the elements of the anti-inflammatory and Mediterranean diets, emphasizing high intake of fruits, vegetables, and whole grains along with low intake of red meat. This could be used as both a general dietary recommendation and in the setting of specific diagnoses such as hypertension and dyslipidemia.
Diets for weight loss
When patients look for guidance regarding weight loss, it is beneficial to look at their current health issues for clues about focusing on a low-fat versus a low-carbohydrate approach. Decreasing overall calories is, of course, necessary for sustained weight loss, but for patients with diabetes or insulin resistance (an estimated 23% of the U.S. population), a low-carbohydrate diet like the Atkin’s diet may prove most effective for them.[111] For those with normal insulin sensitivity, high-carbohydrate, low-fat diets may prove more effective.[112]
People on low-carbohydrate diets have greater success when eating leaner proteins and avoiding saturated fats. Likewise, those on high-carbohydrate, low-fat diets find increased success when their carbohydrates come primarily from fruits, vegetables, whole grains, and legumes. In this way, the foods we replace carbohydrates or fats with in low-carb and low-fat diets seem to matter more than the diet choice itself. In fact, studies have shown that over time, low-fat and low-carb diets have similar weight loss outcomes.[113]
Summary: The best strategy for long-term weight loss is a sustainable diet. The success of low-carbohydrate and low-fat diets depends on the types of nutrients used to replace carbohydrates and fats.
Remember, it is not so much which diet is chosen but one’s willingness to adhere to it that seems to have the greatest impact on body weight.
Back to Erin
After hearing Erin’s story and engaging in a discussion with her about the impact of nutrition on her well-being, the following recommendations could be made.
Since she has insulin resistance, Erin will likely benefit from a diet where she gets most of her carbohydrates from vegetables, fruits, legumes, and whole grains, with a decreased intake of refined carbohydrates.
To feel more full, she can eat more whole grains. When eating carbohydrates she could choose higher fiber breakfast choices like oatmeal, high fiber bread or toast or make her own healthy granola mix. If, for convenience, she selects a granola bar, a bagel, or chips, it would be best to eat the food with something like nuts or a hard-boiled egg, which can prevent sudden spikes and crashes in her blood sugar through the day.
Fiber will help her feel full, and it delays absorption of glucose and cholesterol and improves satiety. It also helps with constipation.
If possible, she should consider eating fatty cold-water fish that are good sources of DHA and EPA twice weekly and eat eggs that have DHA or take an omega-3 supplement.
It is best to cook with extra virgin olive oil and canola oil instead of corn or other vegetable oils.
Protein does not need to be consumed in high quantities. Erin can eat plant-based proteins such as legumes, beans, whole grains, and soy regularly for health benefits, and consume animal protein just a few times weekly.
Vitamins and minerals are best obtained through eating fruits and vegetables and other nutrient-dense foods. Erin should aim to eat a variety of fruits and vegetables (at least 2 of each daily). Juice is very high in sugar and low in fiber and therefore is not recommended as a serving of fruit. She can eat as many non-starchy vegetables as she wants.
Eating well does not have to cost a lot of money. Buying food seasonally, buying less expensive fruits and vegetables, and eating at home regularly can make healthy eating affordable.
To make water taste more interesting, Erin can add some fruit, herbs, or vegetables. Lemon water is delicious, and mint-cucumber water is very refreshing in the summer. Tea can also be a healthy choice, if taken without cream or sugar. For more information refer to the “What We Drink” Whole Health tool.
Eating when feeling bored or sad, but not necessarily hungry, happens to many people. Seeing food from a new point of view and learning new techniques to feel more satisfied with the foods one eats are important skills Erin can develop. Review the “Mindful Eating” Whole Health tool to learn more.
Most people do not need multivitamin or mineral supplements if they eat a well-balanced diet.
Anti-inflammatory and elimination diets can help clarify which foods, if any, are causing symptoms like headaches, rashes, fatigue, constipation, or joint pain. Please refer to the “Elimination Diets” Whole Health tool.
After reviewing her options for improved health, Erin found herself drawn to the MOVE! program and its resources. Erin ultimately chose to begin her journey back to a healthy weight by increasing her fruit and vegetable intake to 5 servings daily and eliminating juice drinks from her children’s diets. Her future plans include a trial of eliminating dairy from her diet to see if her headaches and gastritis improve. She will also start a fiber supplement to help with her post-prandial sugars, lipids, and constipation until she ramps up the fiber she obtains through the foods she eats. She is scheduled to see a dietitian in the near future as well.










 Erin is a 35-year-old Navy Veteran and mother of two. Currently, she is overweight, with a body mass index (BMI) of 29. She often feels tired, struggles with constipation, and has some symptoms of gastritis. She also notes frequent migraines and chronic sinus infections. Erin does not have diabetes, but her doctor is concerned because her fasting glucose is elevated, and she has a strong family history of type 2 diabetes.
Erin is a 35-year-old Navy Veteran and mother of two. Currently, she is overweight, with a body mass index (BMI) of 29. She often feels tired, struggles with constipation, and has some symptoms of gastritis. She also notes frequent migraines and chronic sinus infections. Erin does not have diabetes, but her doctor is concerned because her fasting glucose is elevated, and she has a strong family history of type 2 diabetes.