









File a Dental Claim
Dental claims must be filed filed via 837 EDI transaction or using the most current American Dental Association (ADA) form and comply with ADA and specific, VA requirements listed below. In addition to the information contained on this page, please refer to the instructions provided on the ADA website.
American Dental Association (ADA) website > ADA Dental Claim Form
Claims Submission
Please review the "Where To Send Claims" and the "Where To Send Documentation" sections on the File a Claim for Veteran Care page for submission details. If you are submitting a paper claim, please visit the “Filing Paper Claims” section on the File a Claim for Veteran Care page for information about filing paper claims.
Tips for Successful Dental Claim Submission
Field 1. Type of Transaction
Must be “Statement of Actual Services.” If you are seeking authorization for services, please contact your local VA medical center (VAMC).
Field 2. Predetermination/Preauthorization Number
Must contain the authorization/referral number provided on the VA-supplied authorization form. If you do not have an authorization number, please contact the referring VAMC to obtain one. Claims submitted without an authorization/referral number will be denied. Two formats are acceptable: “VAXXXXXXXXXX” or “XXX-XXXXXX-X.”
Field 15. Policyholder/Subscriber ID (Assigned by Plan)
Veterans VA-assigned integrated control number (ICN), 17 alpha-numeric characters (10 digits + "V" + 6 digits) which can be found on the HSRM referral; will also accept Veteran's full 9-digit social security number (SSN) - no dashes, no spaces.
Field 18. Relationship to Policyholder/Subscriber in #12 Above
Must be “Self.”
Field 38. Place of Treatment
Enter the two-digit Place of Service code; a HIPAA standard. Frequently used codes are:
| Place of Treatment | Place of Service Code |
|---|---|
| Office | 11 |
| Home | 12 |
| Inpatient Hospital | 21 |
| Outpatient Hospital | 22 |
| Skilled Nursing Facility | 31 |
| Nursing Facility | 32 |
| Telehealth (aka Teledentistry) | 02 |
CMS Place of Service Code Set
All current codes are available online from the Centers for Medicare and Medicaid Services (CMS).
Field 49. National Provider Identifiers (NPI) Billing and Field 54. NPI Treating
The Billing and Treating NPI is required on all claim submissions. The NPI is an identifier assigned to HIPAA-covered providers by the federal government.
Field 56. Treatment Location
The physical location where the treatment was rendered. Must be a street address; cannot be a Post Office Box.
Dental Claim Form Completion Aide
The ADA Dental Claim Form provides a common format for reporting dental services to a patient's dental benefit plan. ADA policy promotes use and acceptance of the most current version of the ADA Dental Claim Form by dentists. The ADA Dental Claim Form contains data items required for claim submission. Other data items are conditionally required.
The following sample claim is provided as a reference. All yellow highlighted fields are required. Incomplete or erroneous information will result in claim rejection. All green highlighted fields may be required or become required as the result of input into another field.
Sample Form with Highlighted Fields
Yellow highlighted fields (required) include the following sections:
- Header information: Fields 1 and 2
- Dental Benefit Plan information: Field 3
- Policy holders/Subscriber information: Fields 12 through 15
- Patient information: Field 18
- Record of Service provided: Fields 24, 29, and Fields 30 through 32
- Ancillary claim/treatment information: Field 38
- Billing dentist or dental entity: Fields 48, 49, and 51
- Treating dentist and treatment location information: Fields 53 through 56
Green highlighted fields include the following sections:
- Other coverage: Fields 4 and 5, and Fields 8 through 11
- Patient ID/Account number: Field 23
- Record of service provided: Fields 25 through 28, and Fields 29a, 29b, 34 and 34a
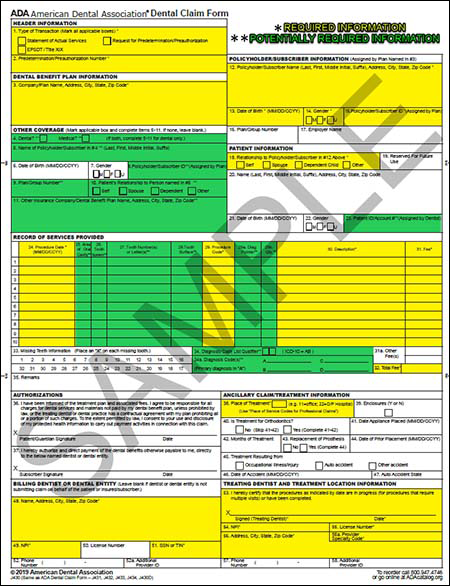
Please click on the image to see a full-sized sample form.






